
Neuroanatomy — MCQs

On this page
To which of the following thalamic nuclei do the spinothalamic fibers project?
All of the following are present in the lateral sulcus except?
Which of the following is not a part of the epithalamus?
All of the following form the deep venous system of the brain, EXCEPT?
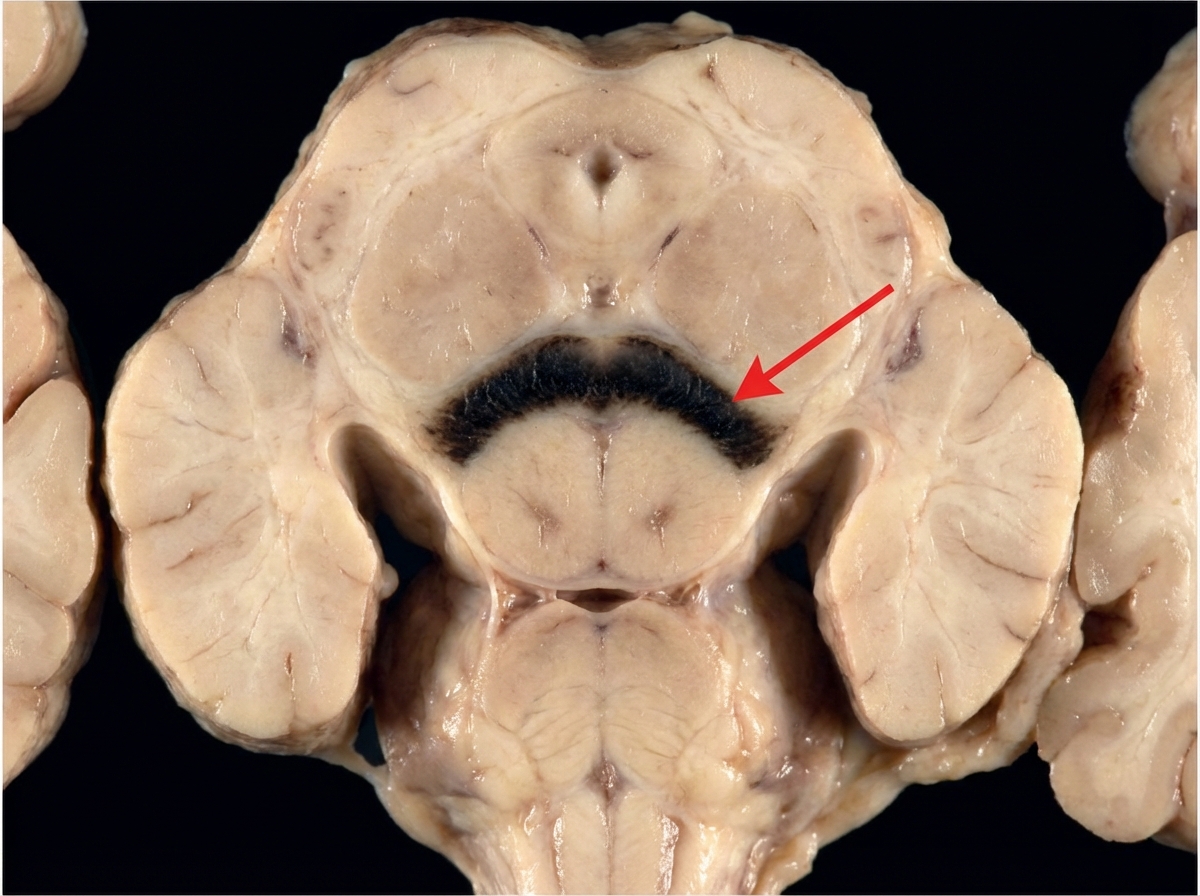
The marked structure is involved in which pathology?
A 58-year-old man is admitted to the emergency department with progressive unilateral hearing loss and ringing in the affected ear (tinnitus) of 4 months' duration. Radiographic examination reveals a tumor at the cerebellopontine angle. Which of the following nerves is most likely affected?
What are the first-order neurons of the anterior spinocerebellar tract?
Which of the following statements is true regarding the nuclei of the 3rd cranial nerve?
Which of the following are components of the Upper Motor Neuron (UMN)?
Which cranial and sacral nerves carry parasympathetic fibers?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app