
Neuroanatomy — MCQs

On this page
On Congo red staining, amyloid appears as what color?
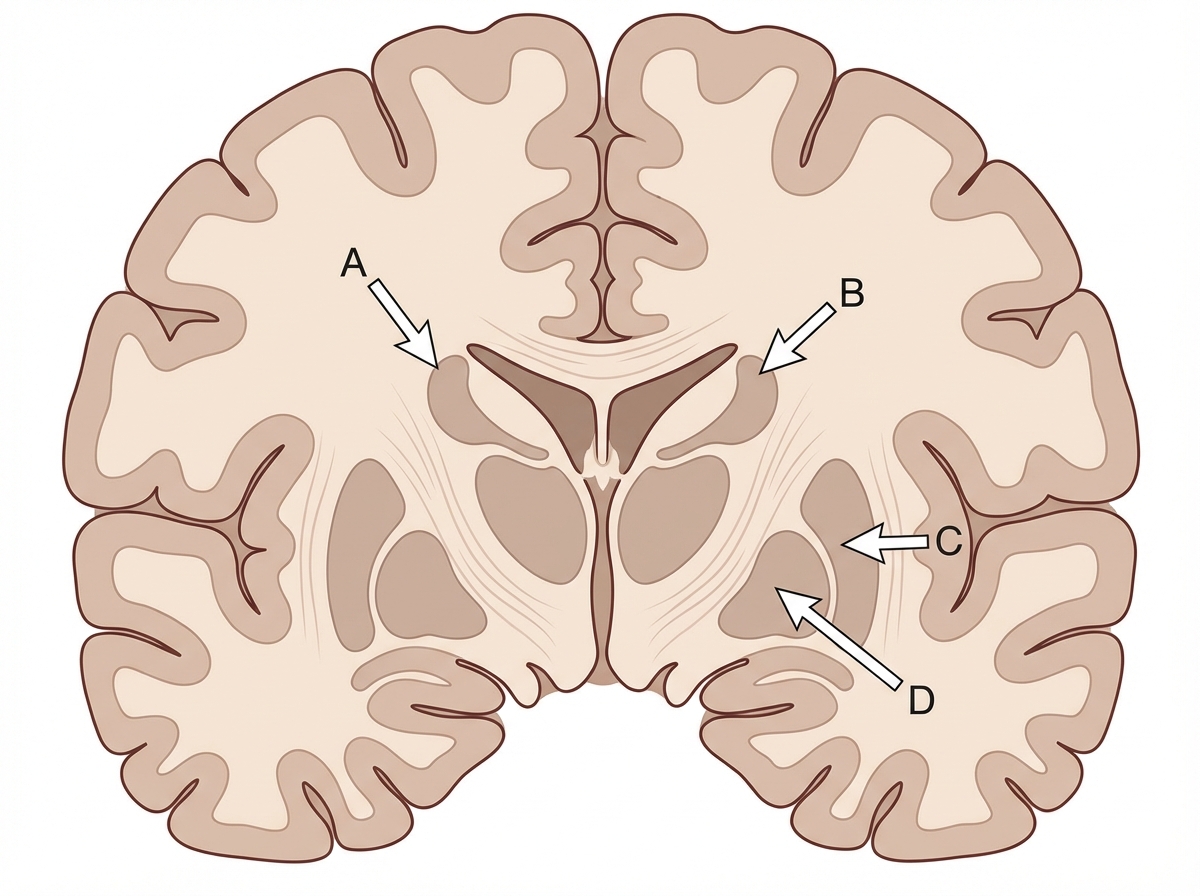
Identify the structure labeled as Caudate nucleus in the given image.
From which structure do the internal arcuate fibres of the medulla originate?
The sternocleidomastoid muscle is supplied by all of the following arteries except?
What is the action of 20mcg/kg/min dopamine?
Which of the following is the largest branch of the vertebral artery?
Which of the following is a DNA repair defect?
What cells form the blood-brain barrier?
What is the recommended maintenance level of mixed venous oxygen saturation in a patient in shock?
From which pharyngeal pouch does the pharyngeal tonsil develop?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app