
Neuroanatomy — MCQs

On this page
Taste sensation from anterior part of tongue is mediated by:
All of the following are true about grey communicans except:
TRUE regarding upper motor neuron VIIth nerve paralysis is:
Auditory pathway is mediated by:
Lesion of facial nerve at level of stylomastoid foramen leads to:
Blood supply to spinal nerve roots is derived from?
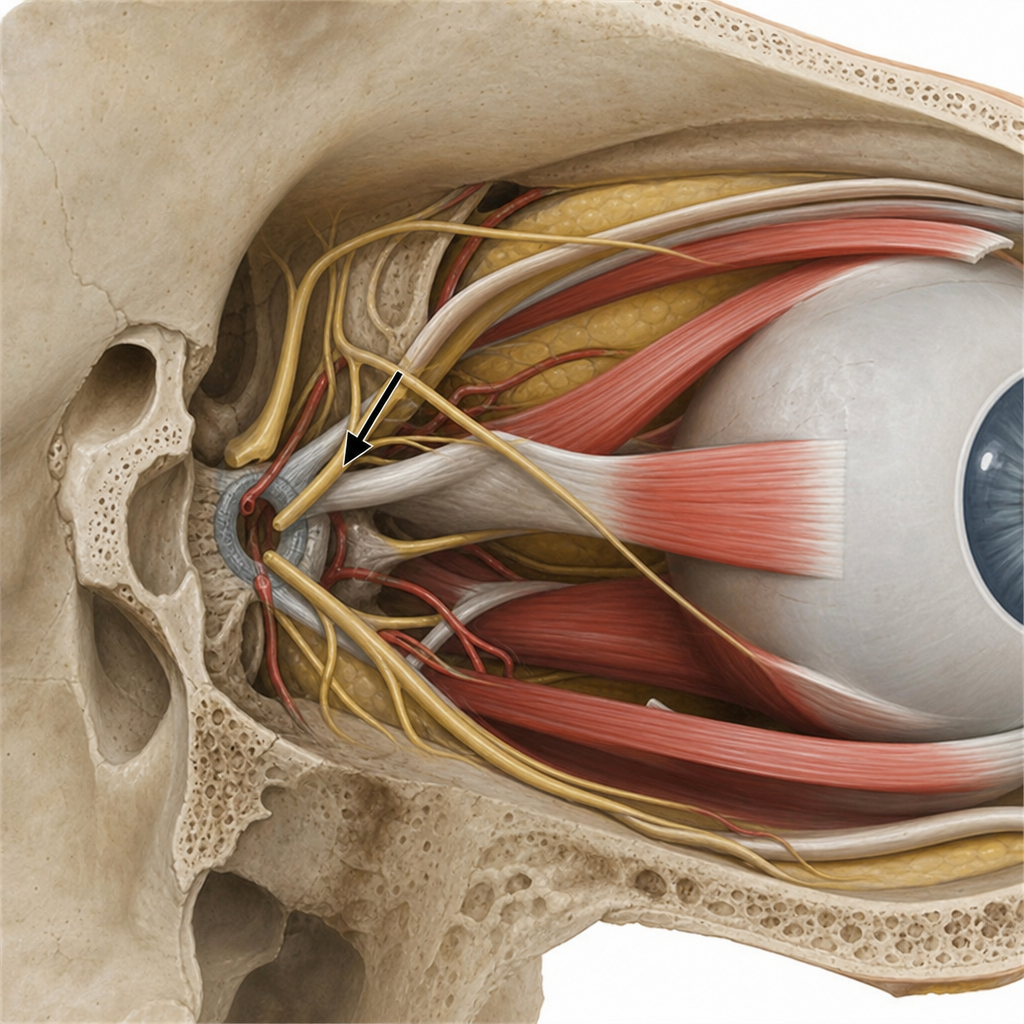
Lesion of the marked structure affects all EXCEPT
The cell body of general somatic and visceral sensory neurons is located within the
Ptosis results from trauma to which nerve?
In postnatal period the greatest growth in the CNS is of?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app