
Neuroanatomy — MCQs

On this page
Which nerve is called the nerve of Wrisberg?
Which muscle is innervated by the Abducens nerve?
A 45-year-old patient presents with difficulty reacting to bright light. On examination, the pupillary light reflex is absent but the near reflex is preserved. Where is the lesion likely located?
A corneal wisp test was performed, and the corneal reflex was elicited. Which of the following nerves is responsible for the afferent limb of this reflex?
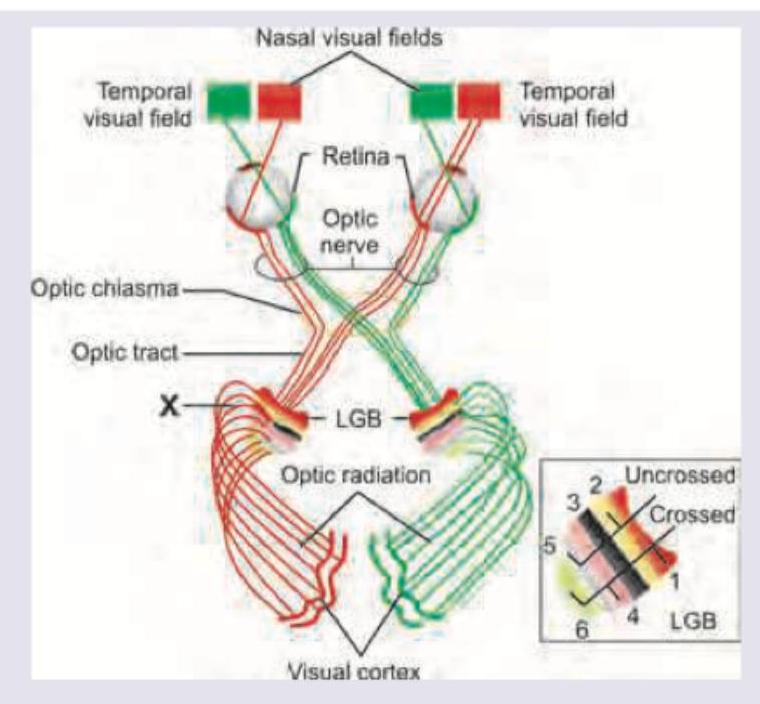
Which of the following lesions will develop after lesion in the area marked as $X$ ?
Arrange the following in the sequence of auditory pathway: 1. Cochlear nucleus 2. Spiral ganglion 3. Superior olivary nucleus 4. Inferior colliculus 5. Medial geniculate body
Match the following: A) Glossopharyngeal nerve B) Spinal accessory nerve C) Facial nerve D) Mandibular nerve 1) Shrugging of shoulder 2) Touch sensation from the posterior one-third of the tongue 3) Chewing 4) Taste from the anterior two-thirds of the tongue
A 45-year-old patient presents with difficulty speaking and swallowing following a stroke. MRI reveals an infarct in the medulla. Which of the following cranial nerve nuclei is most likely affected?
During an examination of the cranial nerves, a patient shows inability to move their eye laterally past the midline. Which of the following structures in the cavernous sinus is most likely affected?
Which part of thalamus is related to motor control?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app