
Neuroanatomy — MCQs

On this page
Which part of the brain is supplied by the anterior cerebral artery?
Cerebellar connections to other parts of the brain are projected through which type of cell?
Which of the following is NOT included in the cerebellar nuclei?
What is true about the spinal cord?
In Bogorad syndrome, where does damage to the parasympathetic fibres of the facial nerve occur?
Special visceral efferent innervation does NOT involve which of the following structures?
A young woman presents with neurological deficits following an explosion. She has no movement in her right lower extremity with hyperreflexia, loss of proprioception and fine touch in this extremity, but pain and temperature sensation are intact. Pain and temperature sensation are absent in the left lower limb. Movement and reflexes are normal in the left lower extremity and upper extremities. A lesion in which of the following locations can explain her neurological examination?
General visceral fibres do not supply which of the following structures?
Which of the following is NOT a branch of the intracranial part of the Internal carotid artery?
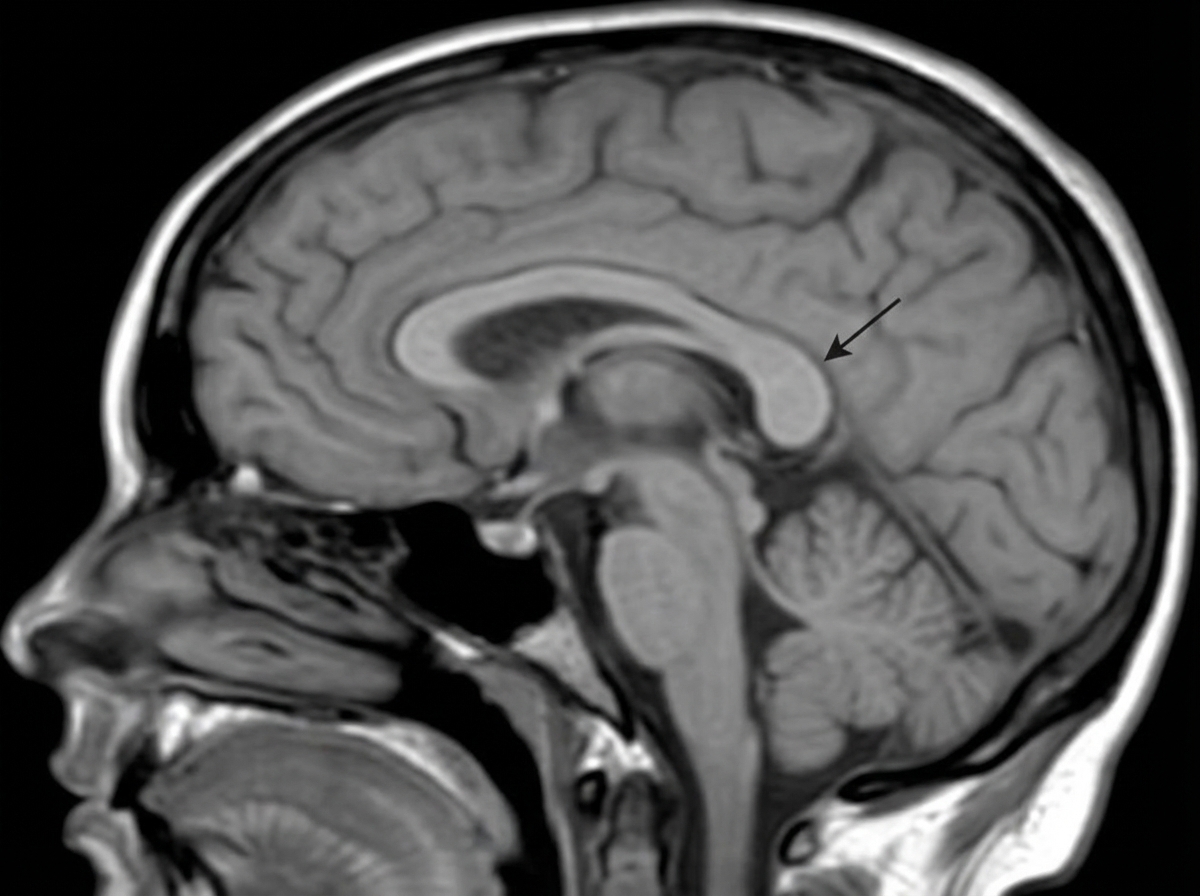
Identify the structure indicated by the arrow in the corpus callosum.
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app