
Neuroanatomy — MCQs

On this page
Which of the following cells are NOT present in the cerebellar cortex?
Which of the following is NOT a nucleus of the basal ganglia?
What type of nerve ending is characteristic of nuclear bag fibers?
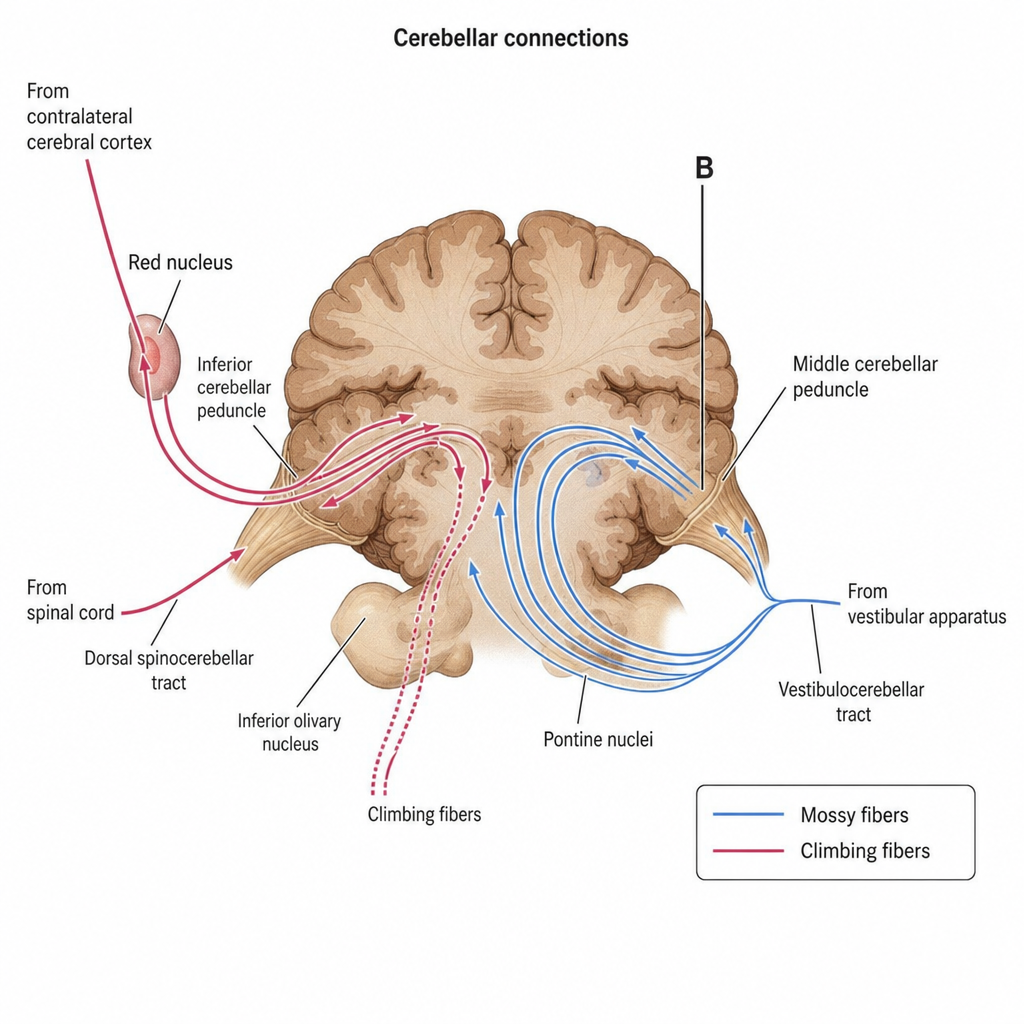
Structure B is formed by which tract?
General visceral afferent fibres do not supply which of the following?
At what cervical spinal cord level is the circumference maximum?
Unilateral trigeminal nerve injury is tested by:
Birbeck granules are characteristic of which cell type?
Which nerves comprise the parasympathetic nervous system?
The sympathetic trunk rests on which part of the vertebra?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app