
Neuroanatomy — MCQs

On this page
A neurological examination of a 47-year-old woman reveals a normal corneal reflex in her right eye, but no consensual corneal reflex in her left eye. Which of the following additional findings might be expected?
Which of the following is NOT a division of the Vth cranial nerve?
Pseudounipolar neurons are typically found in which of the following locations?
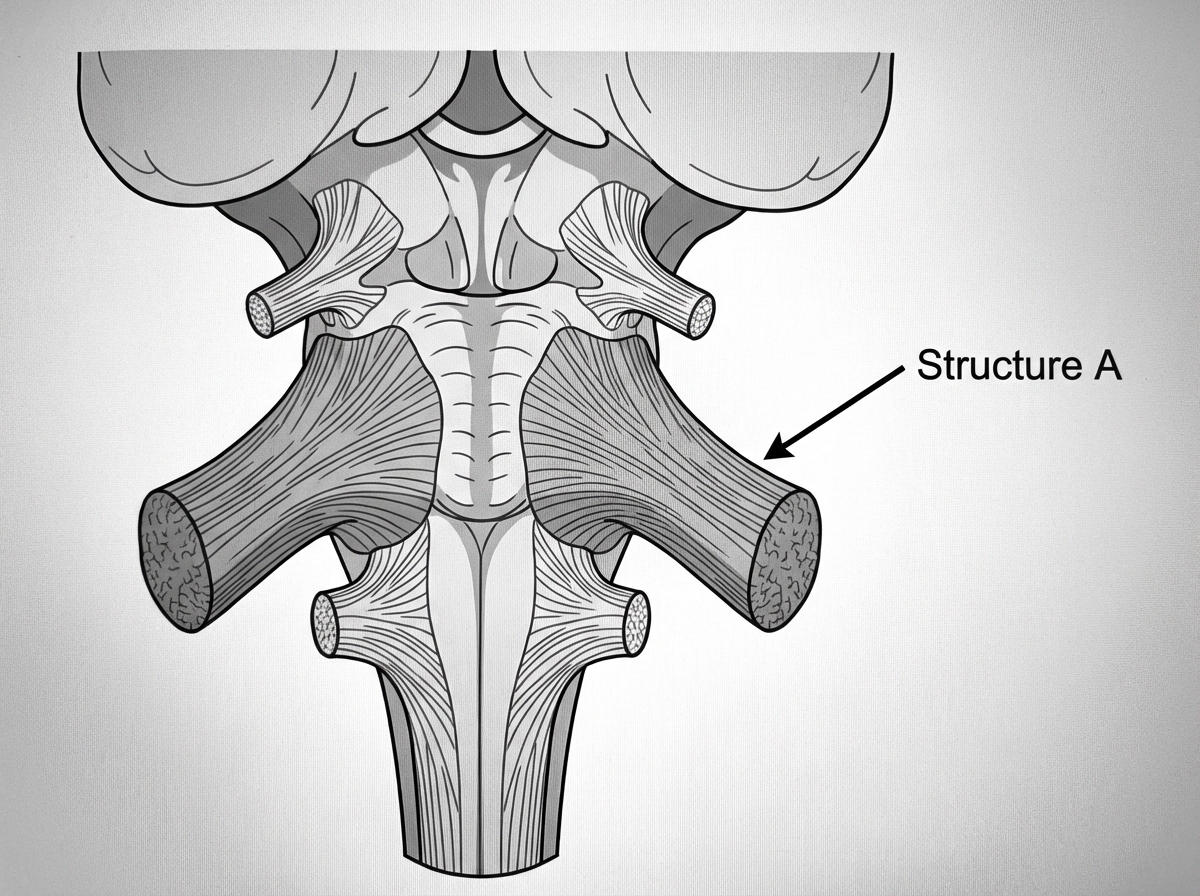
Structure A is formed by which of the following tracts?
In a lesion of the right hypoglossal nucleus, which way does the tip of the tongue turn on protrusion?
Which of the following tracts is seen in the posterior column of the spinal cord?
All of the following are parts of the optic nerve except?
After graft repair of a thoraco-abdominal aneurysm, a patient is unable to move both lower limbs. What is the most probable cause?
What is Charcot's artery?
Vertebral arteries of both sides unite to form which of the following arteries?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app