
Neuroanatomy — MCQs

On this page
Eye examination of a patient revealed lack of upward gaze and dilated pupils fixed to light. What is the MOST probable location of the lesion?
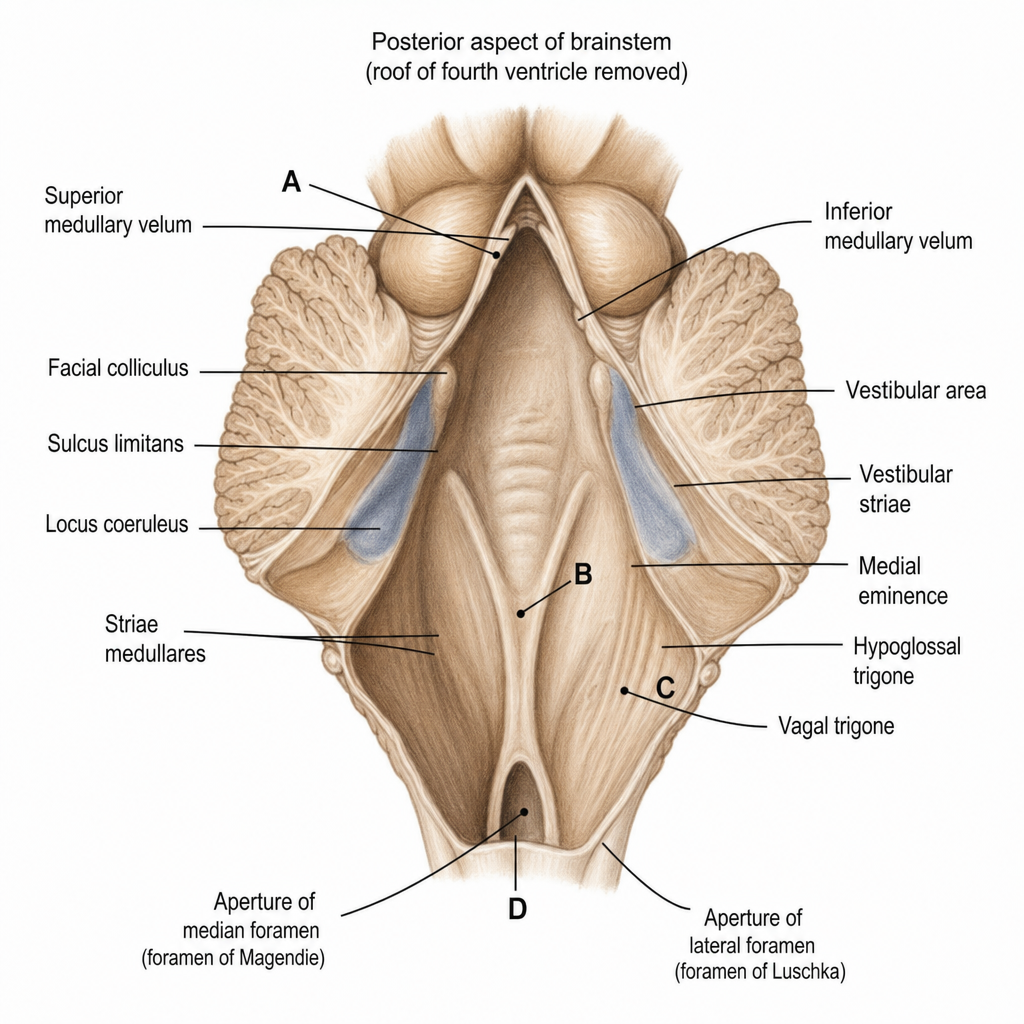
Which of the following markers denotes the lateral recess of the fourth ventricle?
A 65-year-old woman with diabetes mellitus presents for examination. When the right side of her pharynx is touched with a tongue blade, the palate elevates symmetrically. However, when the left side of the pharynx is touched, the palate does not elevate at all. Which of the following cranial nerves is most likely responsible for this finding?
A 35-year-old male cannot adduct his left eye while looking to the right. Where is the lesion located?
All of the following are derivatives of the Mullerian duct except?
Wallerian degeneration includes which of the following processes?
Fetal alcohol syndrome comprises of which of the following features?
Which is the deep nucleus of the cerebellum?
Crocodile tears syndrome, characterized by spontaneous lacrimation during eating due to misdirection of regenerating autonomic nerve fibers, occurs after injury to which of the following nerves?
All of the following statements about the vagus nerve are true EXCEPT:
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app