
Neuroanatomy — MCQs

On this page
When are the axons of the corticospinal tracts fully myelinated?
Which structure(s) in the cerebellum has/have a topographical representation of the body?
The superior cerebellar peduncle primarily carries which of the following types of fibers?
Which of the following is unlikely to be involved in a lesion of the anterior spinal artery?
Absorption of cerebrospinal fluid (CSF) primarily occurs through which anatomical structure?
Which cranial nerve emerges from the dorsal aspect of the brainstem?
Proprioceptive fibers are not carried by which cranial nerve?
Severe pain that arises after injury to or sectioning of a peripheral sensory nerve is called as?
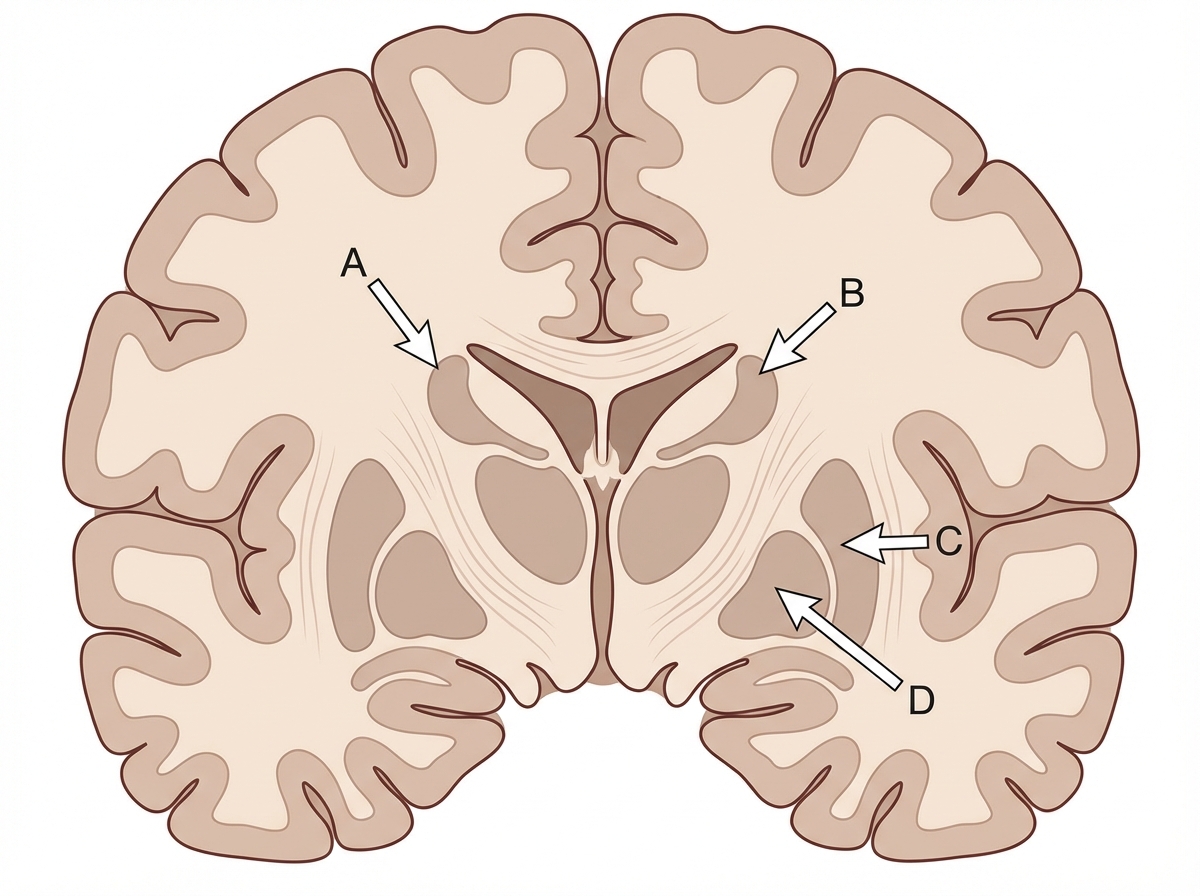
Identify the structure labeled as Caudate nucleus in the given image.
From which structure do the internal arcuate fibres of the medulla originate?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app