
Neuroanatomy — MCQs

On this page
Which nucleus in the brain is common to the IX, X, and XI cranial nerves?
General visceral fibres do not supply which of the following structures?
Which of the following is NOT a branch of the intracranial part of the Internal carotid artery?
Paradoxical splitting of the second heart sound is heard in which of the following conditions?
Cell matrix adhesion are mediated by?
How many nuclei does the trigeminal nerve have?
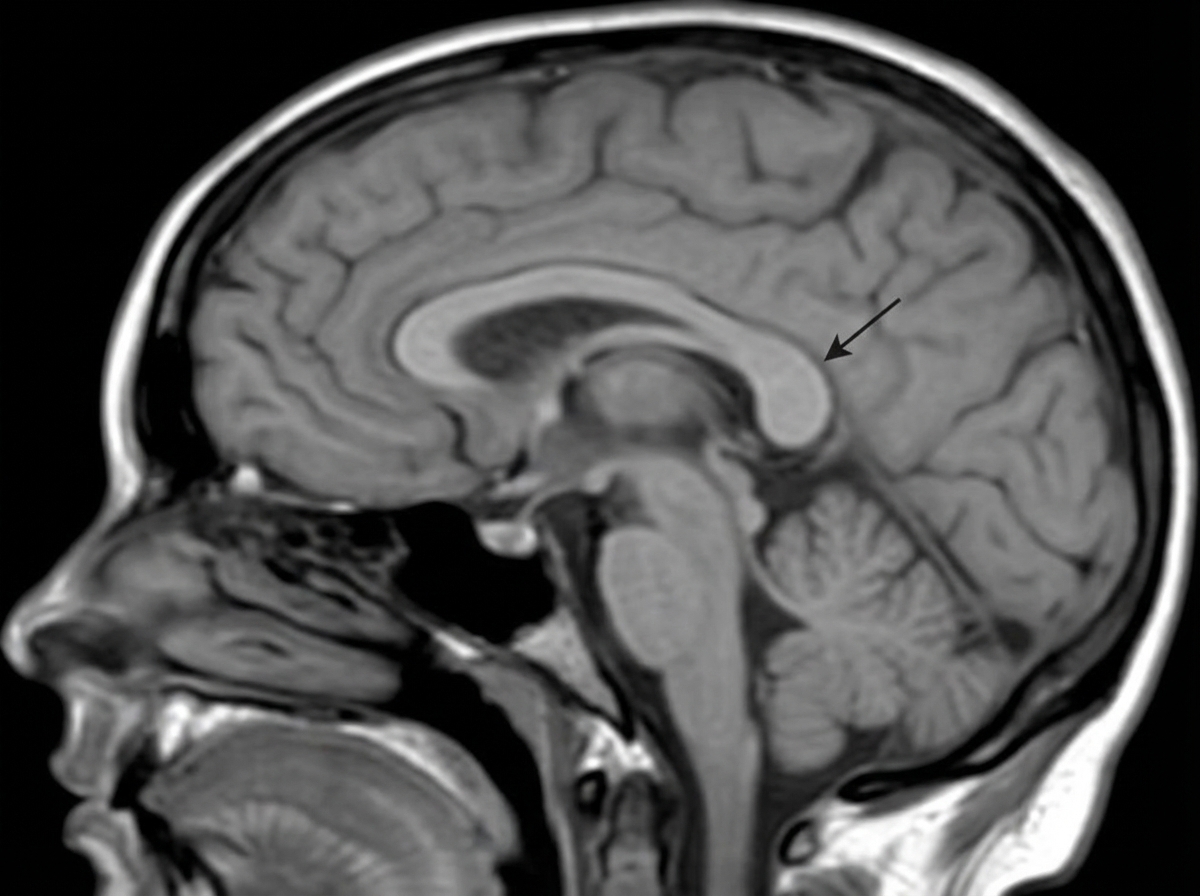
Identify the structure indicated by the arrow in the corpus callosum.
Lateral Medullary Syndrome involves all of the following cranial nerves, EXCEPT:
Which is the most prominent spinous process?
An apical lung tumor can cause which of the following signs?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app