
Neuroanatomy — MCQs

On this page
A 34-year-old male complains of hyperacusis (sensitivity to loud sounds). Injury to which of the following cranial nerves is responsible?
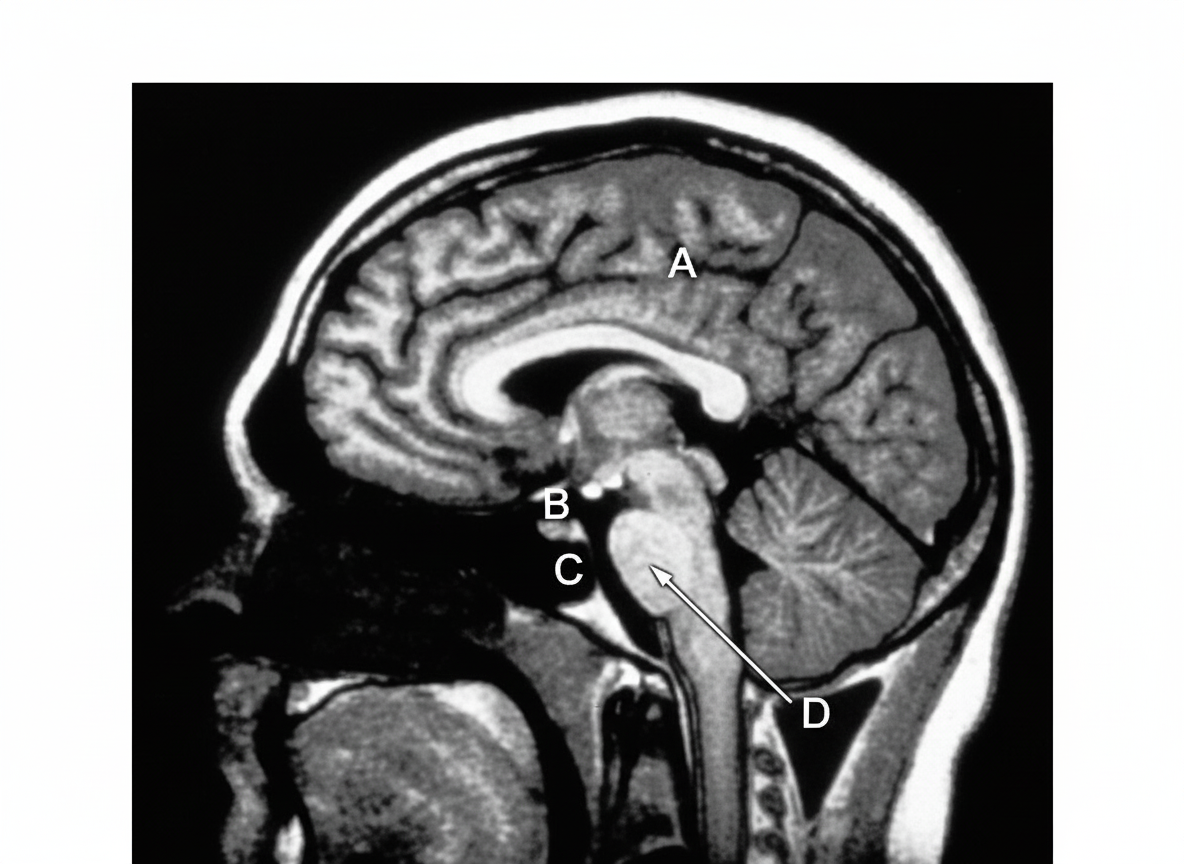
T1 weighted MRI of midsagittal section of the brain is shown. Which among the marked structures contains the two lateral foramina of Luschka?
Which of the following is an oncogenic RNA virus?
Trismus is due to spasm of which muscle?
Which of the following muscles is supplied by two nerves?
All the following structures have a Blood-Brain Barrier except?
What is the name of the junction of the anterior horn and posterior horn of the lateral ventricle?
All of the following structures pass through the superior orbital fissure EXCEPT:
A 'blow-out fracture' of the orbit most commonly involves which part?
Which cranial nerve is the second cranial nerve?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app