
Neuroanatomy — MCQs

On this page
Which of the following is not a mixed nerve?
Blockage of which of the following blood vessels leads to the medial medullary syndrome?
The dorsal root ganglion contains which of the following?
Which of the following are common types of posterior mediastinal tumors?
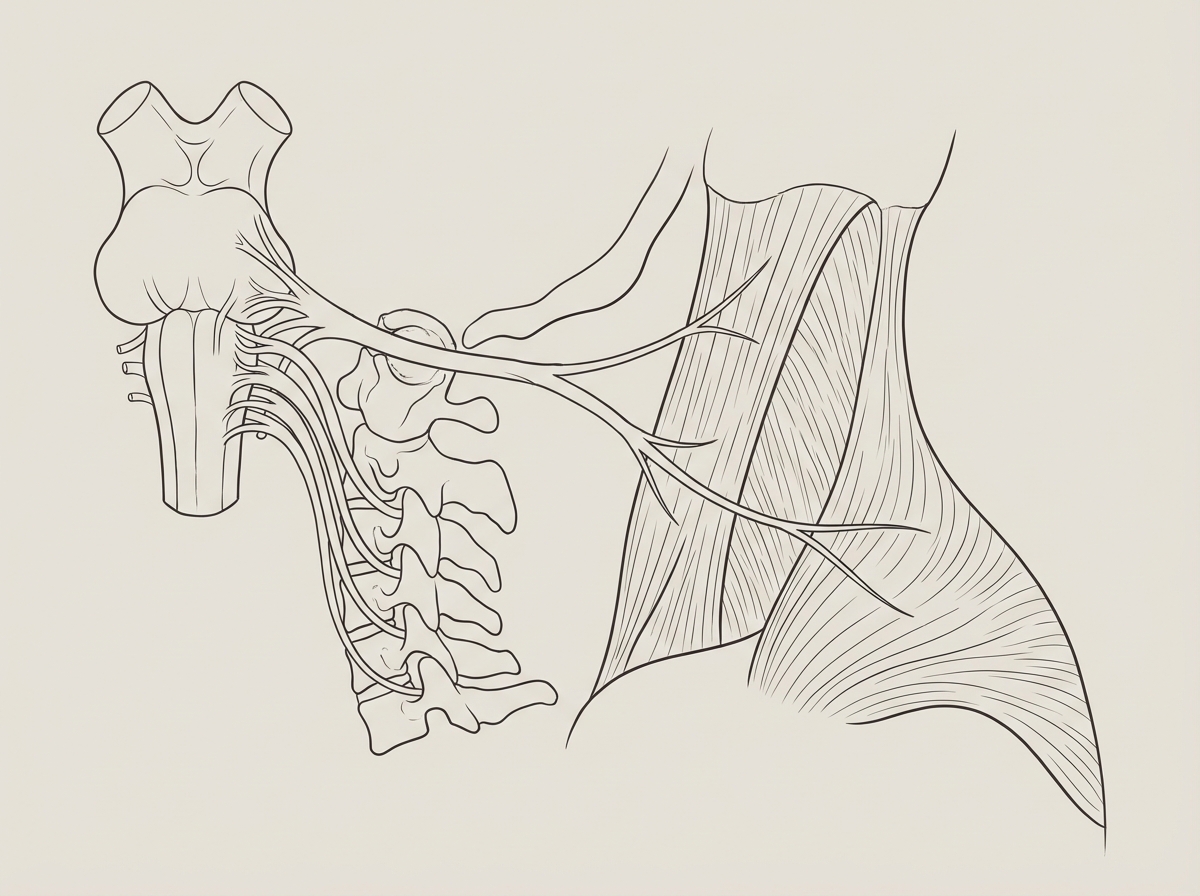
Which cranial nerve is shown in this diagram?
All of the following are true about Arnold Chiari Malformation Type I except:
Climbing fibres originate from which nucleus?
In which of the following parts does the VIIth nerve take the narrowest path during its entire course?
What type of neuron is present in the autonomic ganglion?
Which of the following structures is insensitive to pain?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app