
Neuroanatomy — MCQs

On this page
What is a known side effect of vagal nerve stimulation?
A patient cannot speak but can communicate by writing. Which of the following brain areas is most likely affected?
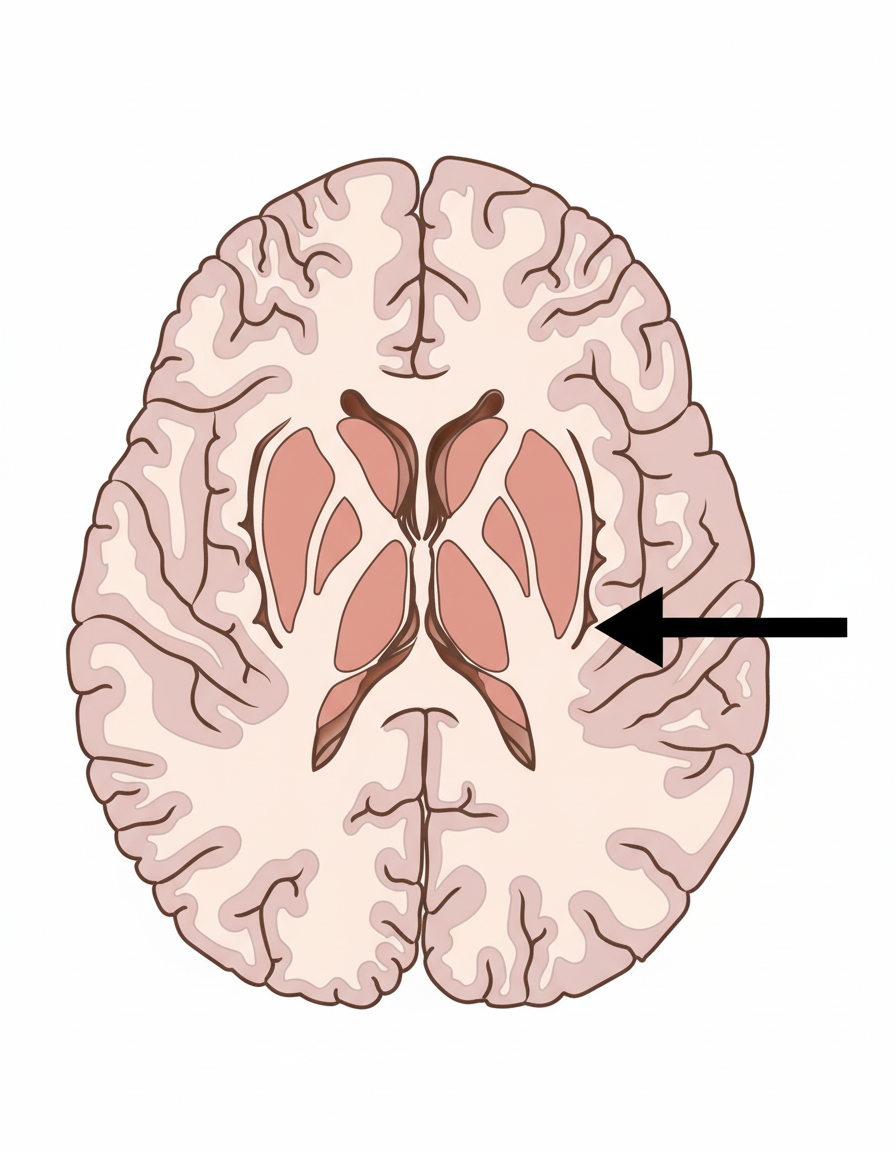
Identify the structure located at the position indicated by the arrow within the internal capsule.
Which of the following is a finding of trigeminal nerve injury?
Which of the following cranial nerves are pure motor nerves?
The red nucleus is present at which level of the brainstem?
What is the earliest microscopic change indicative of neoplastic transformation?
Which of the following statements regarding the medial longitudinal fasciculus (MLF) is incorrect?
Preganglionic fibres to the submandibular ganglion arise from which nucleus?
Which of the following is NOT a part of the limbic system?
Practice by Chapter
Organization of the Nervous System
Practice Questions
Spinal Cord Anatomy
Practice Questions
Brainstem Anatomy
Practice Questions
Cerebellum
Practice Questions
Diencephalon
Practice Questions
Cerebral Cortex
Practice Questions
Basal Ganglia
Practice Questions
Limbic System
Practice Questions
Cranial Nerves
Practice Questions
Autonomic Nervous System
Practice Questions
Neural Pathways and Tracts
Practice Questions
Neurovascular Anatomy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app