
Lower Limb — MCQs

On this page
Inversion of the foot is produced by which of the following muscles?
Which of the following forms the tendinous sling in the superficial arch of the foot?
Tibialis posterior has insertion to all of the following bones except?
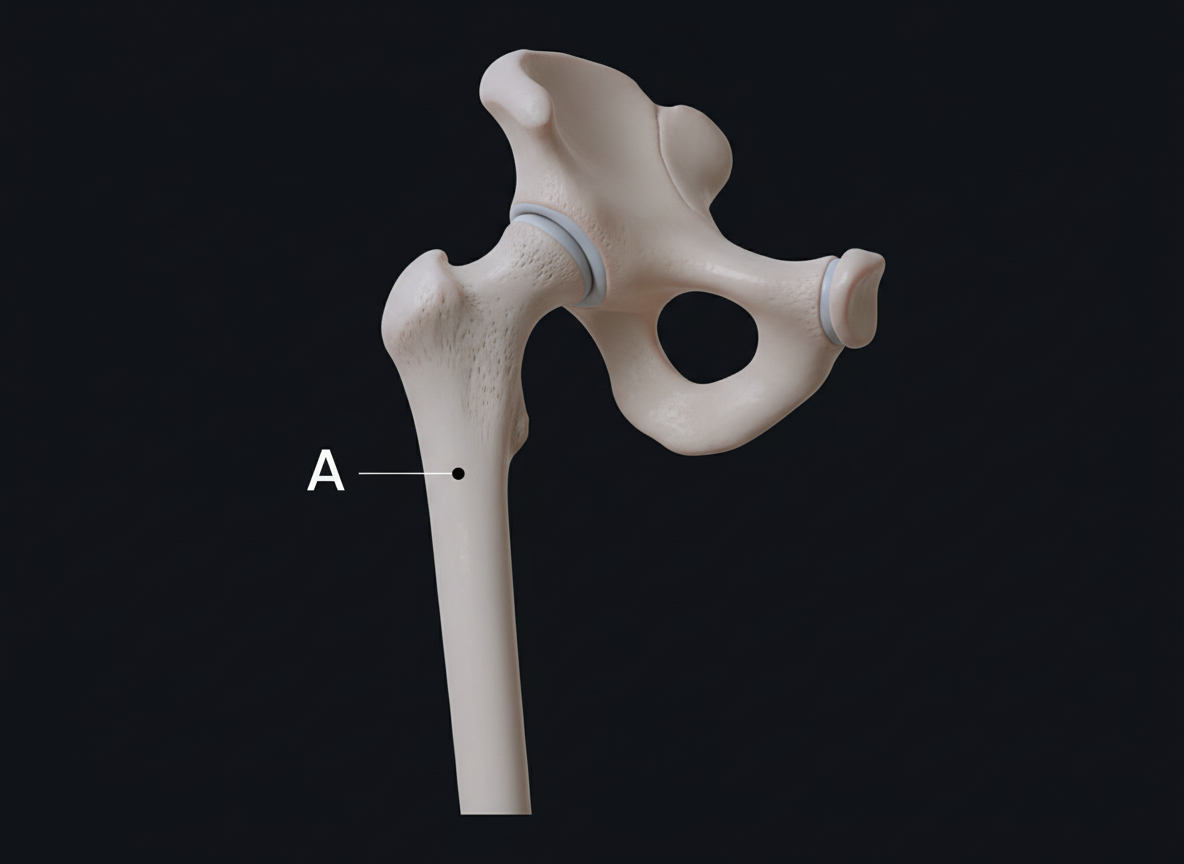
Identify the muscle that does not insert on the structure marked A.
During the surgical repair of a femoral hernia, which structure is most vulnerable to major injury?
What is the origin of the Posterior Cruciate Ligament (PCL)?
The obturator nerve innervates all of the following muscles except?
A 45-year-old male presents with fractures of the tibia and fibula after a bicycle fall. On physical examination, he has a foot drop but normal foot eversion. Which of the following nerves is most likely injured?
What is the nerve supply of the obturator internus muscle?
Which tarsal bone articulates with the tibia and fibula?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app