
Lower Limb — MCQs

On this page
The Trendelenburg sign is due to paralysis of which muscle?
Which muscle of the foot is NOT supplied by the lateral plantar nerve?
What is the most anterior structure on the tibial plateau?
Which muscle, primarily acting as an evertor of the ankle, inserts into the medial cuneiform?
Venous return to the heart during quiet standing is facilitated by all of the following factors EXCEPT?
Which muscle is supplied by the lumbar plexus?
Which of the following statements is true regarding the posterior cruciate ligament?
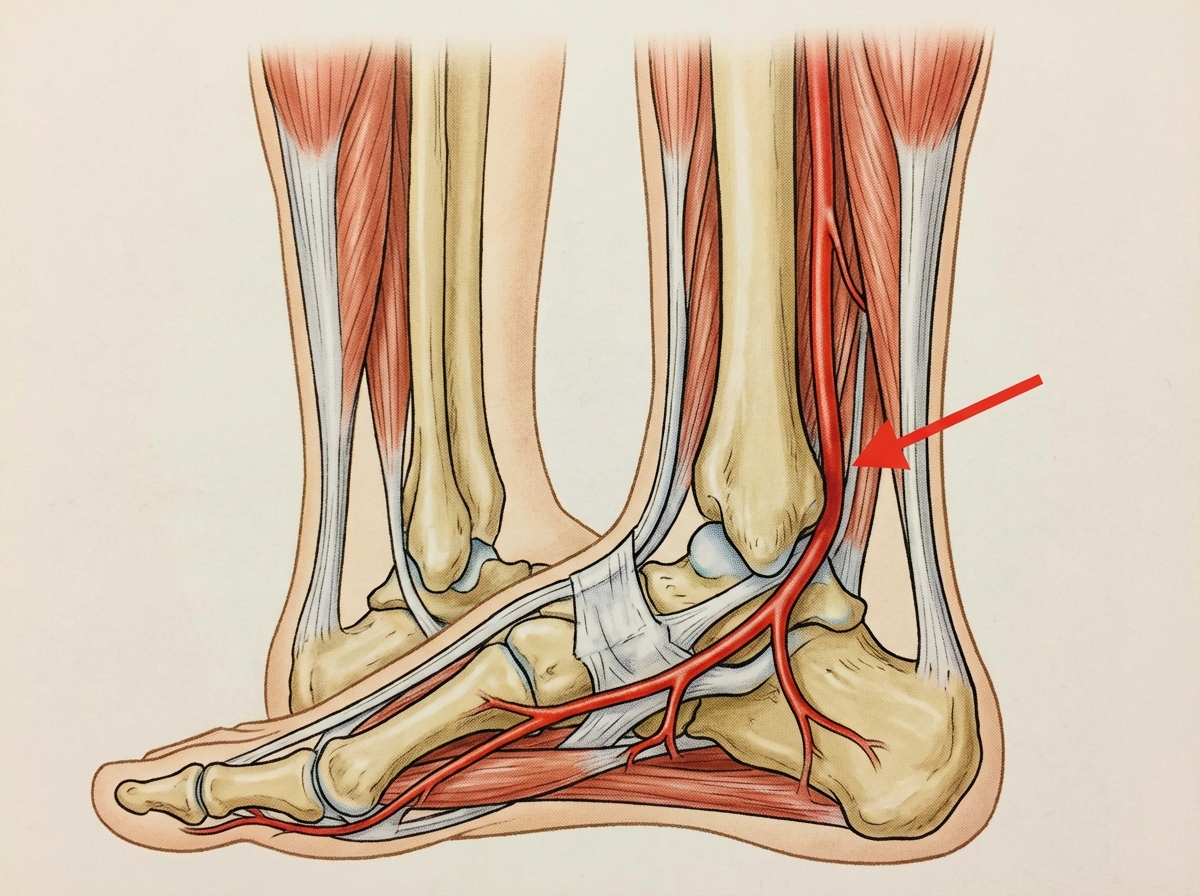
What is the name of the marked artery?
Which of the following is NOT TRUE about the Iliotibial tract?
What is the nerve root value for the knee jerk reflex?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app