
Lower Limb — MCQs

On this page
What is true about the cuboid bone?
The popliteal artery is difficult to palpate because:
Which nerve supplies the adductor compartment of the thigh?
Which of the following is NOT true regarding the course of the great saphenous vein?
What is the largest synovial joint in the body?
Which of the following tendons is commonly used for transplantation in the body?
A patient sustained a hyperextension injury to the knee. Which of the following ligaments prevents excessive anterior gliding of the femur on the tibia?
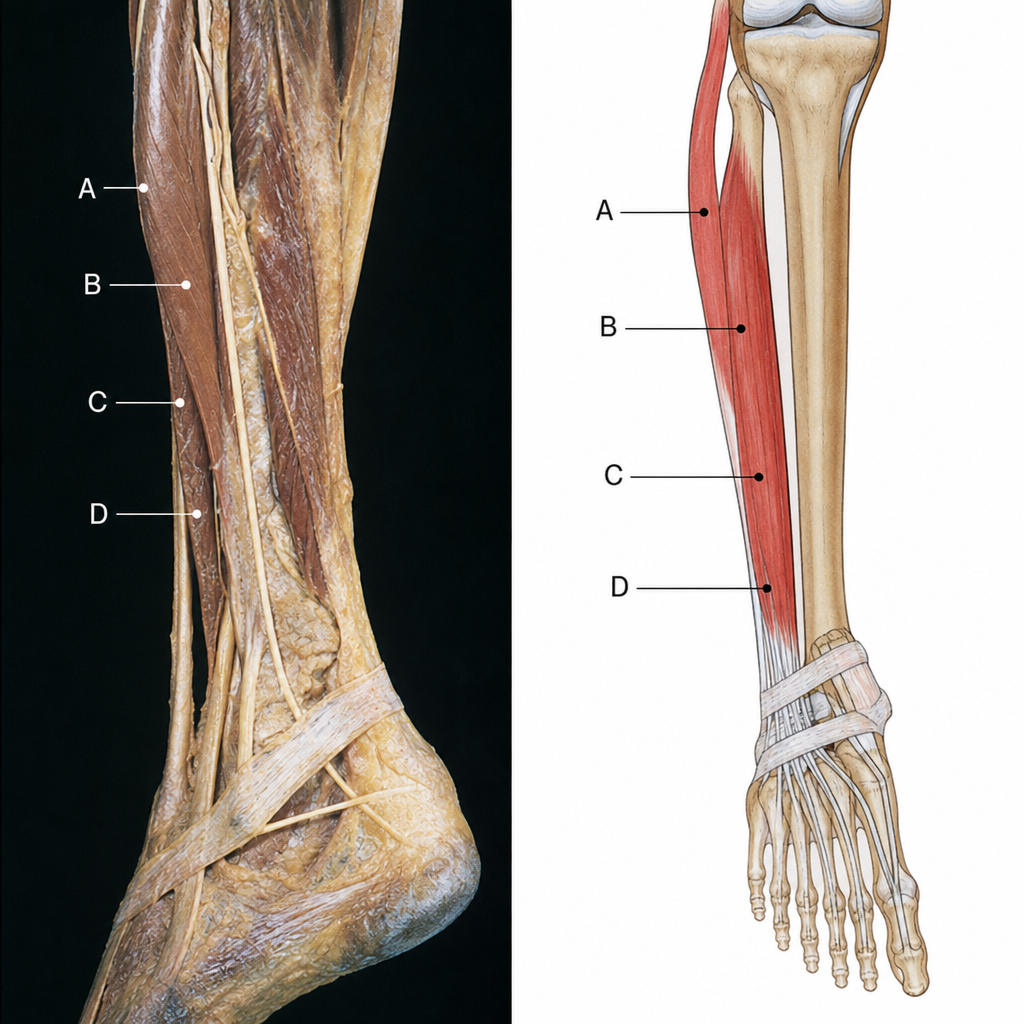
A 20-year-old male suffered trauma to his right leg while playing football and did not seek medical attention initially. The affected area became painful, red, and tender. A few days later, he noticed he had to drag the affected foot, and examination revealed a loss of eversion along with foot drop, consistent with injury to the common fibular nerve as it winds around the neck of the fibula. Which of the labeled muscles in the image is fibularis (peroneus) longus?
What is the chief extensor of the knee joint during hip flexion?
A sesamoid bone is present in the tendon of which of the following muscles?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app