
Lower Limb — MCQs

On this page
Which structure(s) passes behind the inguinal ligament:
Tibialis posterior is inserted in all of the following bones distally, except for which of the following?
Tarsal tunnel syndrome involves
Which of the following muscles inserts into the rough impression on the anterior surface of the greater trochanter?
Which of the following nerves does not supply the muscles of the gluteal region?
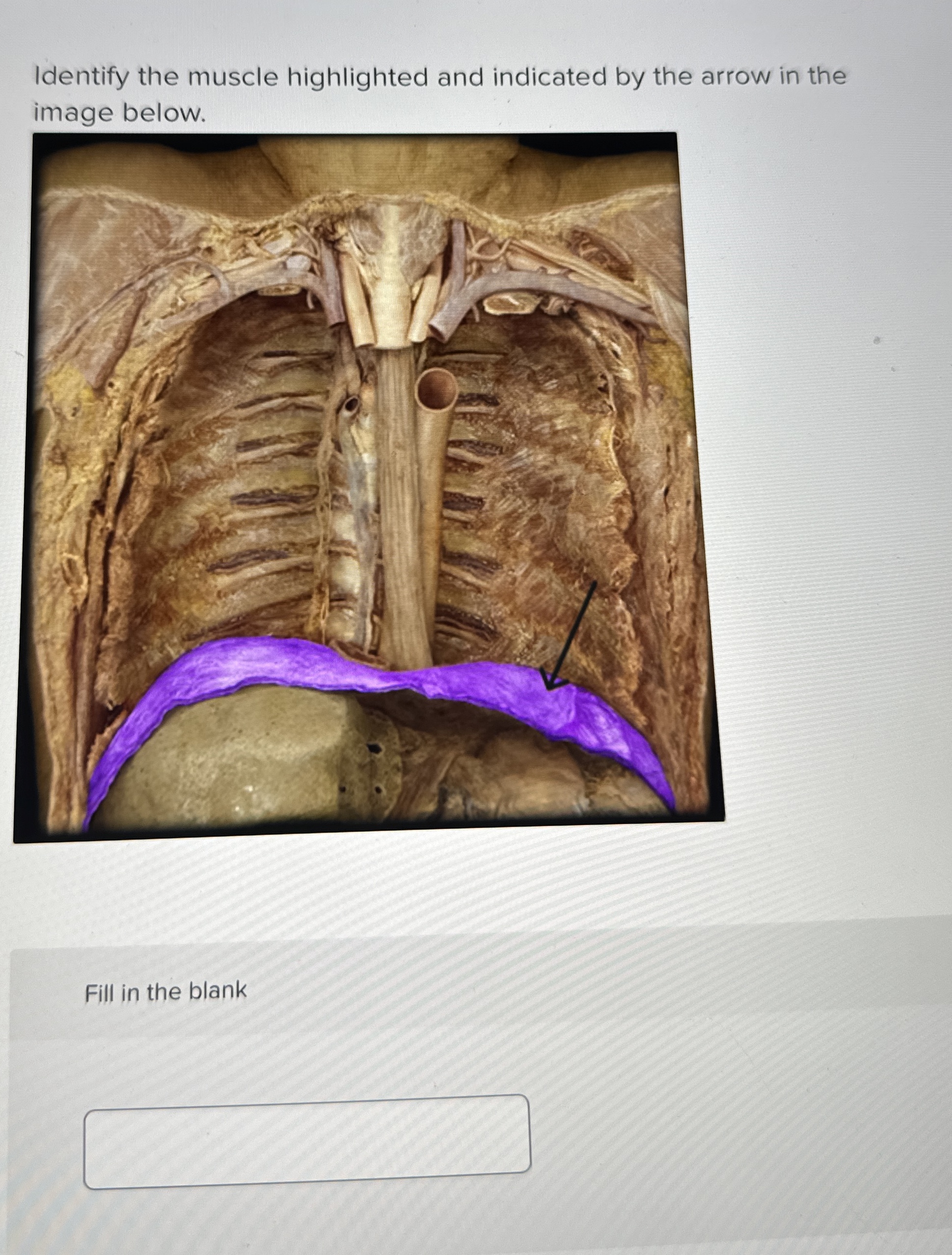
Name the marked structure in the image.
All are possible during contraction of the tensor fasciae latae muscle except.
Which of the following statements about the adductors of the thigh is correct?
Which metatarsal is known for its significant mobility in the foot?
Which structure passes deep to the inguinal ligament in the vascular compartment?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app