
Lower Limb — MCQs

On this page
What is the PRIMARY action of the muscle marked in the image?
Which muscles are supplied by the superficial peroneal nerve?
A patient presents with meralgia paresthetica. Based on the diagram, identify the nerve involved in this condition.
Which is correct about the markings shown on the left popliteal fossa? (Recent NEET Pattern 2016-17)

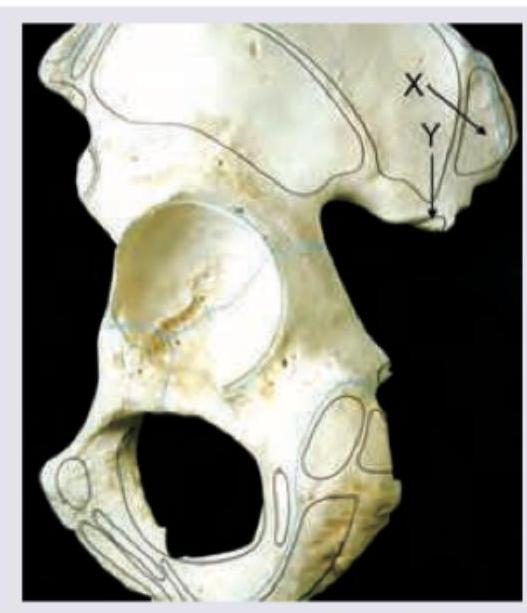
The image shows left hip bone lateral surface. Name the muscle attached at X and the muscle passing through Y respectively:
Identify the bone marked as X.

Femoral hernias are more common in females because :
Consider the following structures in the femoral triangle: 1. Femoral canal 2. Femoral Nerve 3. Femoral artery 4. Femoral vein What is the correct sequence of the above from medial to lateral ?
Sprain of the ankle joint results from an injury to:
Which ligament connects medial cuneiform to the base of the 2nd metatarsal?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app