
Lower Limb — MCQs

On this page
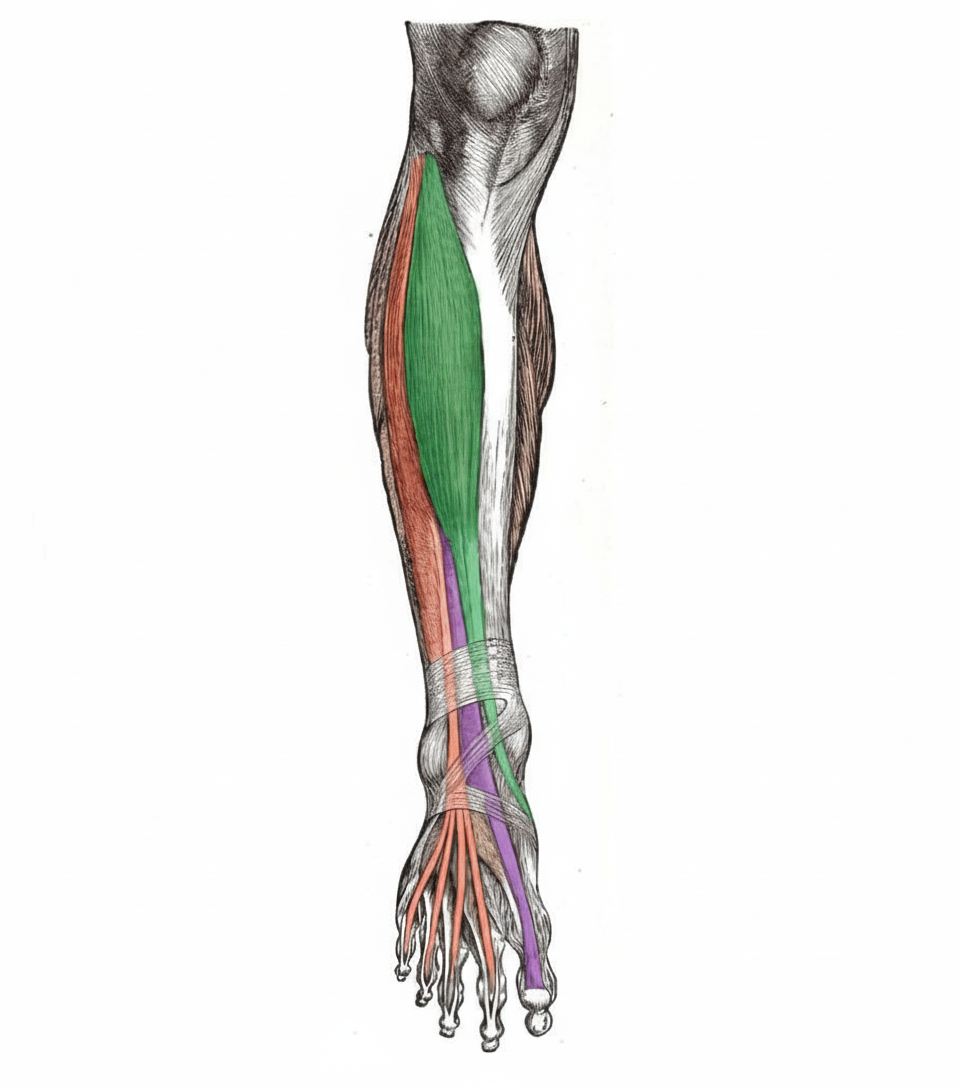
Which nerve supplies the muscle shown in the illustration?
What is true regarding the semitendinosus muscle?
The involvement of the L5 Nerve Root can affect all of the following movements, except?
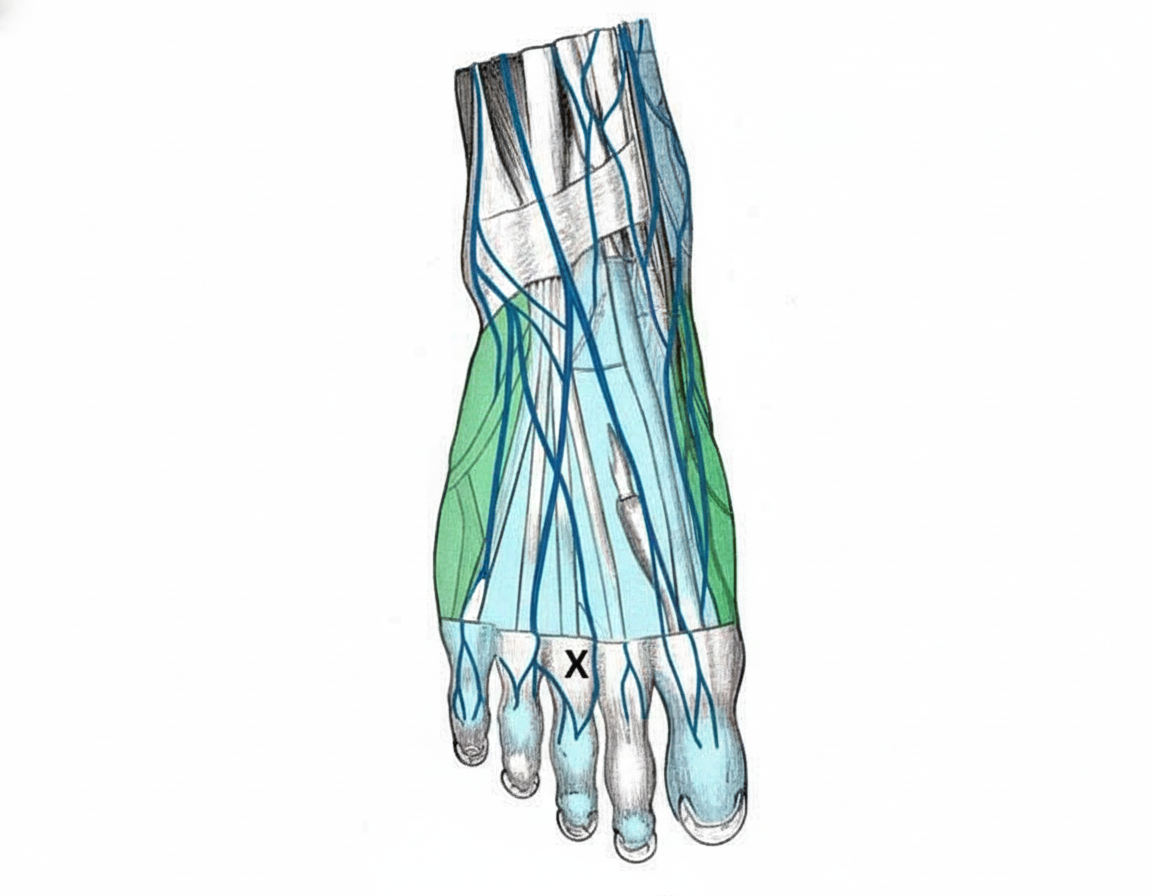
What is the cutaneous nerve supply of the region marked X?
A serious complication of fractures of the femoral neck is avascular necrosis of the femoral head. This usually results from rupture of which artery?
The talus bone articulates with all of the following EXCEPT:
Which of the following is true about attachments at the ischial tuberosity?
Which nerve is most likely to be injured in a posterior dislocation of the hip joint?
The ischial tuberosity provides attachment to which muscle?
A young patient presents with loss of sensation in the sole of the foot and paralysis of the medial side of the plantar muscles of the foot. Most likely nerve involvement is?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app