
Lower Limb — MCQs

On this page
Which is the least mobile metatarsal of the foot?
The femoral sheath contains all except:
A construction worker falls feet-first from a roof. He sustains a fracture of the groove on the undersurface of the sustentaculum tali of the calcaneus bone. Which of the following muscle tendons is most likely torn?
"Anaesthesia on the sole of the foot" is caused by injury to which nerve?
Rider's bone ossifies in which of the following muscles?
Which nerve supplies the skin over the femoral triangle?
Which of the following statements about the great saphenous vein is true?
Which of the following is NOT an abductor of the hip joint?
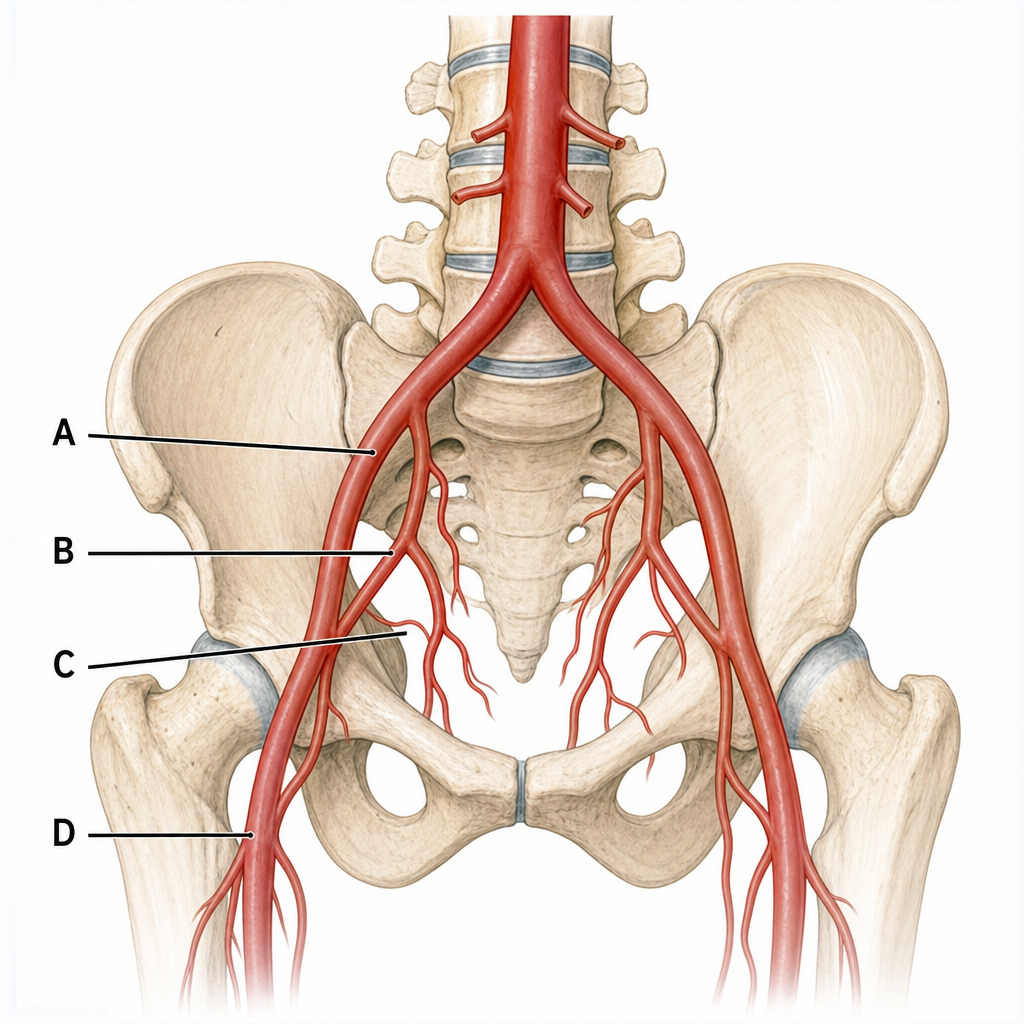
The femoral artery begins at which anatomical landmark?
In which structure would ligation of the external iliac artery reduce blood pressure?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app