
Lower Limb — MCQs

On this page
An athlete is sitting on the edge of a table with knees flexed at 90 degrees. When the athlete fully extends their knee, what happens to the tibial tuberosity in relation to the patella?
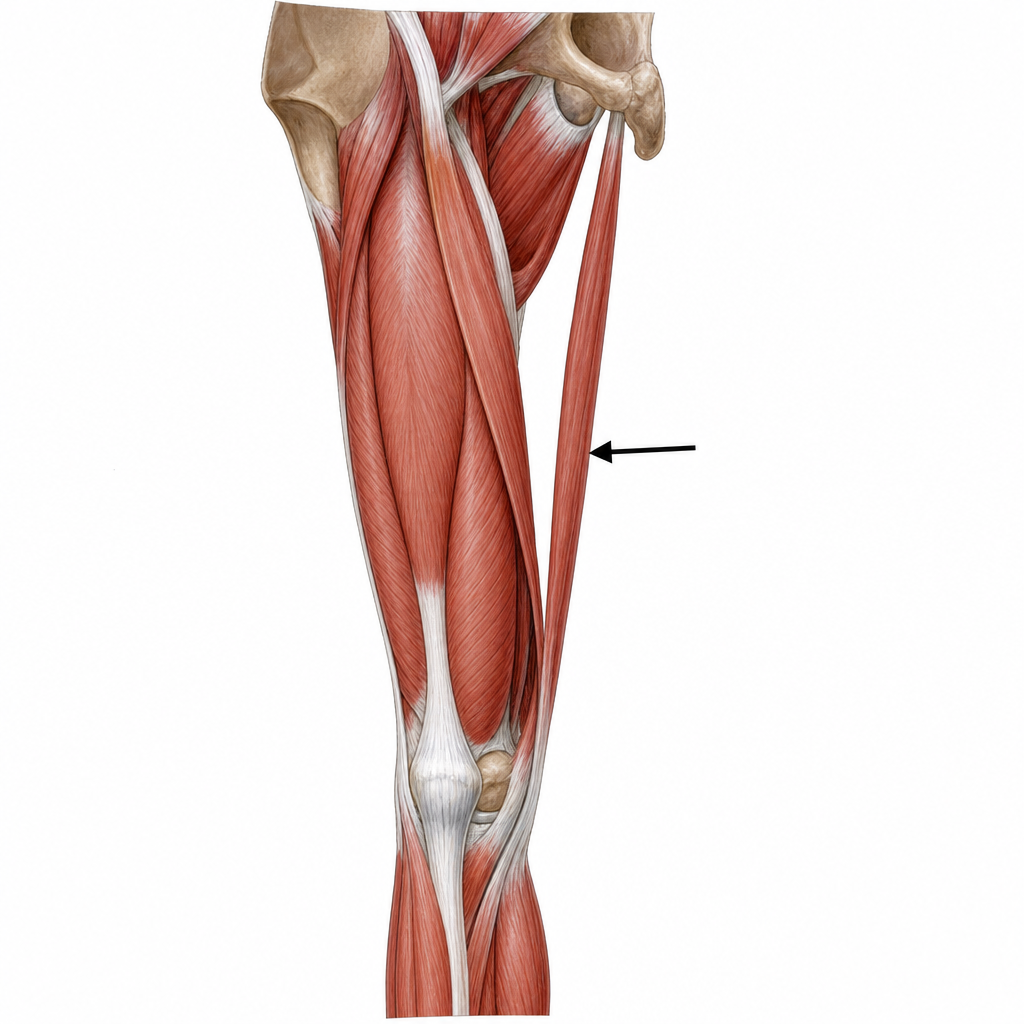
Identify the structure indicated by the arrow in the provided diagram.
All of the following are contents of the adductor canal, EXCEPT?
The condyles of the tibia provide attachment to which of the following?
An 80-year-old man presents with severe pain at his right hip and thigh, with difficulty in standing and reduced mobility. He reports a fall 2 days prior and a 3-year history of steroid use. An MRI of the right hip was performed. Which artery is most likely injured, leading to this condition?
A 17-year-old boy was stabbed, resulting in the transection of the obturator nerve. Which of the following muscles is completely paralyzed?
A 22-year-old man presents after a bicycle accident with a tibial fracture above the ankle. Physical examination reveals a severed tibial nerve on the posterior aspect of the tibia. Which of the following signs will most likely be present during physical examination?
A 49-year-old man presents with a cold and pale foot. Physical examination reveals peripheral vascular disease, with duplex ultrasound studies indicating possible occlusion of his popliteal artery and an absent posterior tibial artery pulse. What is the most common location for palpation of the posterior tibial artery pulse?
The base of the femoral triangle is formed by which anatomical structure?
A 56-year-old male with advanced bladder carcinoma suffers from difficulty while walking. Muscle testing reveals weakened adductors of the right thigh. Which nerve is most likely being compressed by the tumor to result in walking difficulty?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app