
Lower Limb — MCQs

On this page
A 55-year-old man is admitted to the hospital for an iliofemoral bypass. The operation is performed successfully and the blood flow between the iliac and femoral arteries is restored. During rehabilitation, which of the following arteries should be palpated to monitor good circulation of the lower limb?
Inversion and eversion of the foot occur at which joint(s)?
Which compartment of the leg is devoid of a neurovascular bundle?
The nutrient artery to the femur is a branch of which of the following?
Which of the following is a compound condylar joint?
The posterior cutaneous nerve of the thigh supplies the skin overlying which of the following areas?
During physical examination of a patient with a history of TIA, the ankle jerk reflex is found to be absent. Which of the following nerves is responsible for this reflex arc?
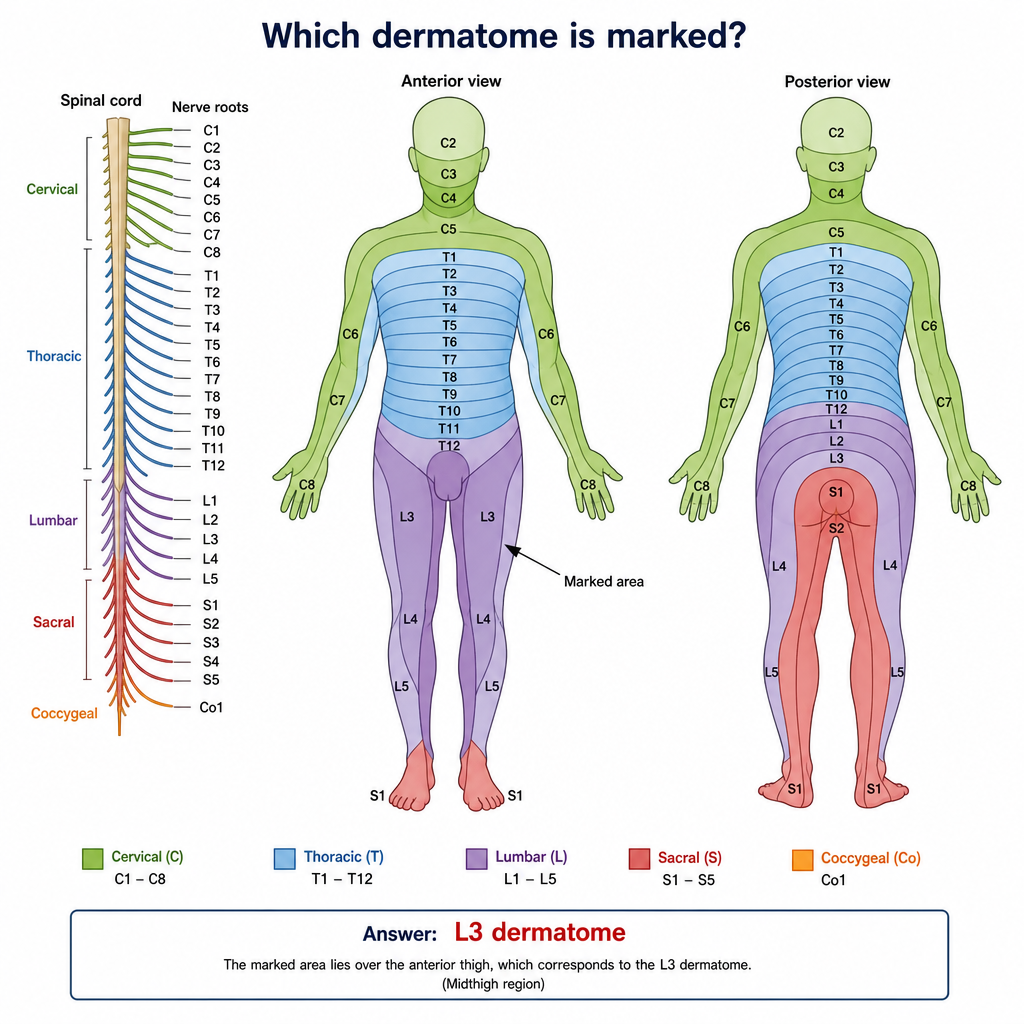
Which dermatome is marked?
Which of the following muscles is NOT supplied by the deep peroneal nerve?
Which of the following is NOT a muscle of the first layer of the foot?
Practice by Chapter
Gluteal Region and Hip
Practice Questions
Thigh and Popliteal Fossa
Practice Questions
Leg and Foot
Practice Questions
Joints of Lower Limb
Practice Questions
Nerves of Lower Limb
Practice Questions
Arterial Supply and Venous Drainage
Practice Questions
Lymphatic Drainage
Practice Questions
Muscles and Their Actions
Practice Questions
Gait Analysis and Biomechanics
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app