
Abdomen — MCQs

On this page
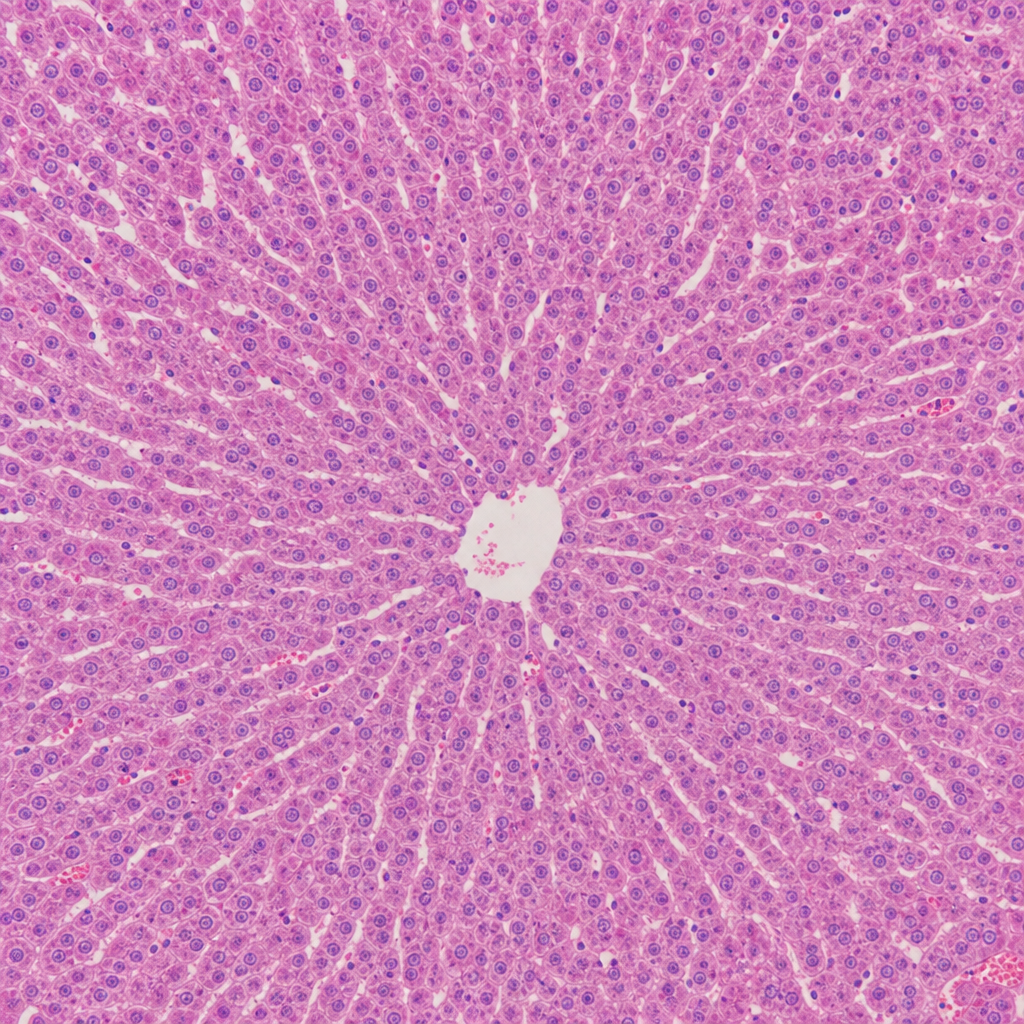
What is the predominant source of blood supply to the organ shown in the histological slide?
Which of the following abdominal structures is responsible for sharp pain during abdominal surgery?
Which anatomic landmark demarcates upper gastrointestinal bleeding from lower gastrointestinal bleeding?
All of the following form the boundary of the left suprarenal gland EXCEPT?
The accessory obturator artery is a branch of which artery?
In case of Inferior Vena Cava (IVC) obstruction, which of the following collateral pathways does NOT open up?
All of the following are true regarding the anatomical relationships of the kidney and ureter, EXCEPT?
What is the lymphatic drainage of the umbilicus?
Other than the spleen, occlusion of the splenic artery at its origin will most likely affect the blood supply to which of the following structures?
How many segments is the liver divided into?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app