
Abdomen — MCQs

On this page
Haustrations are found in which part of the digestive system?
Which of the following is NOT among the contents of the rectus sheath?
Which of the following arteries is a direct branch of the gastroduodenal artery?
What is the ratio of the renal cortex to medulla in adults?
Portocaval (portosystemic) anastomosis is seen at all the following sites EXCEPT?
Which of the following statements about the third part of the duodenum is untrue?
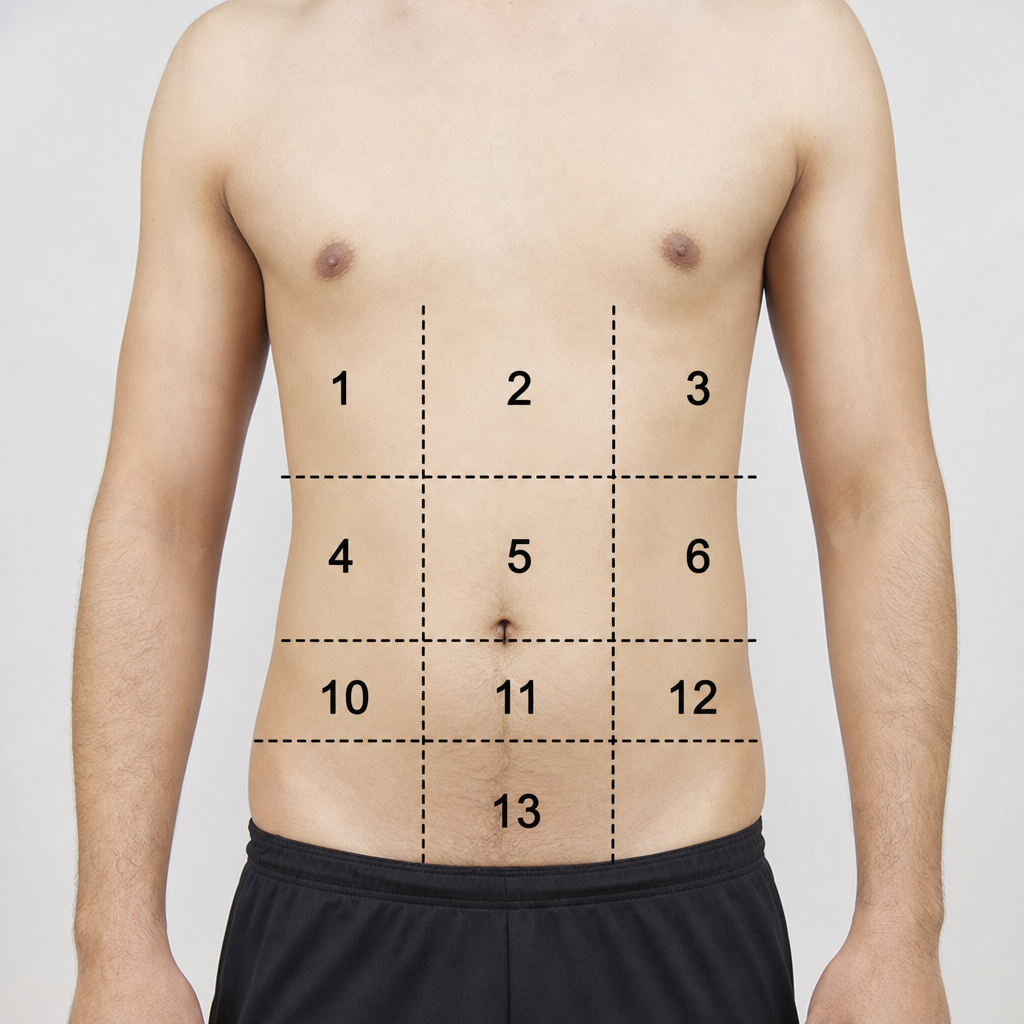
Which number is pointing to the left iliac region?
The gastrosplenic ligament is a peritoneal reflection surrounding which artery?
Which of the following are the main sources of blood supply to the stomach?
The cardiac orifice of the stomach is located at the level of which vertebra?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app