
Abdomen — MCQs

On this page
Lymphatics of the suprarenal gland drain into which group of lymph nodes?
The ligament teres is a remnant of what structure?
What are the blood vessels that supply the stomach?
Which of the following structures does not form the boundary of Hesselbach's triangle?
Identify the structure marked in the image.
Which of the following structures marked in the image contains the splenic artery?
Identify the segment marked in red in the image below.
The ligament of Treitz (suspensory ligament of the duodenum) marks the anatomical boundary between which two structures?
Which of the following is not a boundary of the hepatocystic triangle?
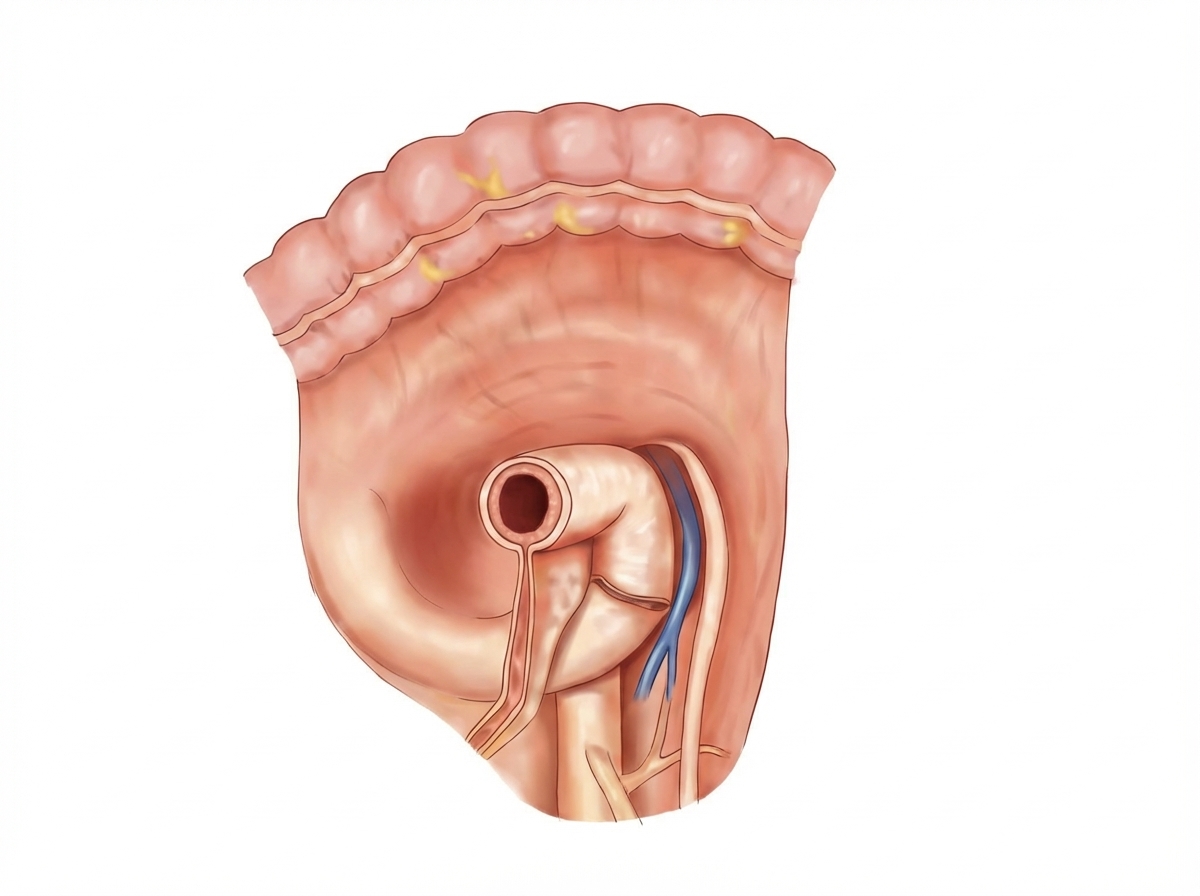
The image shows the para-duodenal fossa region. The para-duodenal fossa is a sickle-shaped fold of peritoneum, sometimes found arching between the left side of the duodeno-jejunal flexure and the medial border of the left kidney. Its right free edge forms the anterior boundary of the para-duodenal recess. Which structure is contained in the right free edge of the para-duodenal fold?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app