
Abdomen — MCQs

On this page
Subdiaphragmatic peritoneum is more absorptive than pelvic peritoneum because the former possesses which of the following?
Which of the following is true about the renal arterial system?
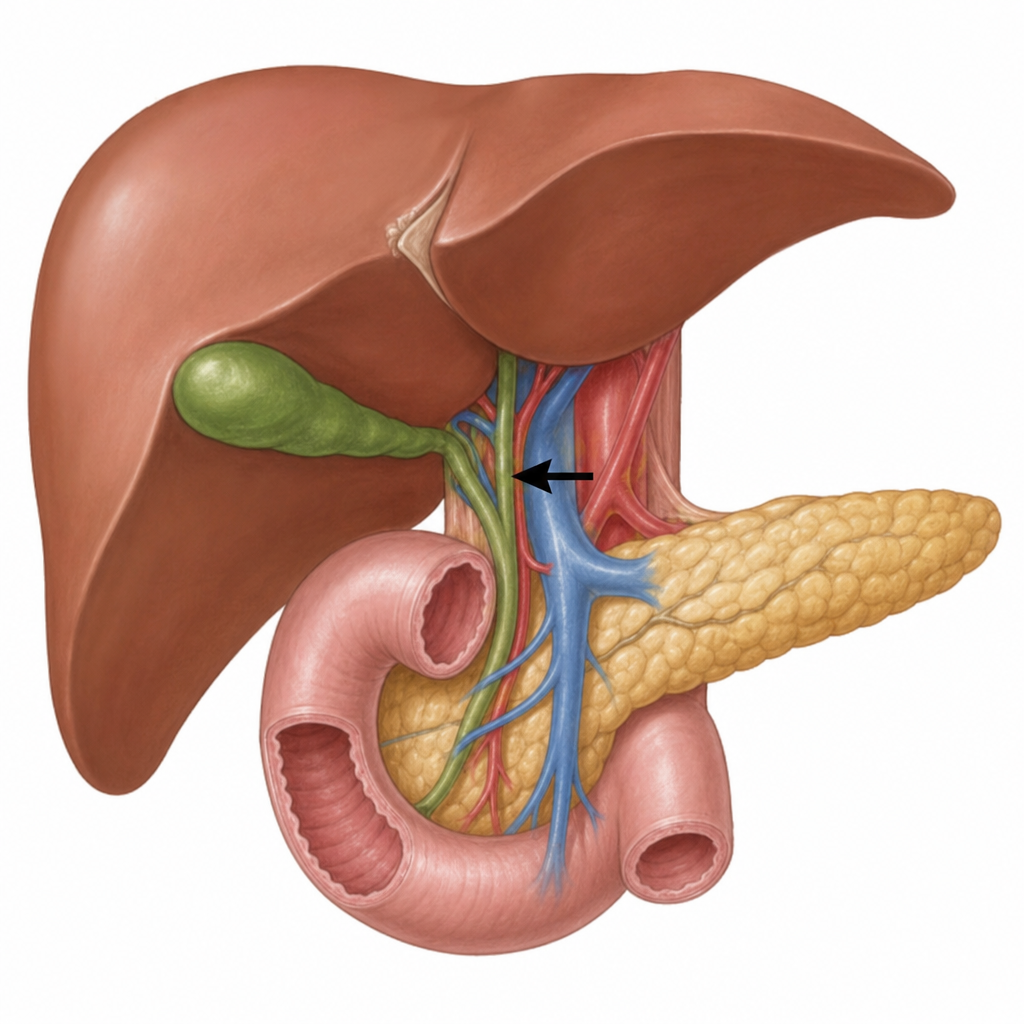
What is true regarding the anterior boundary of the epiploic foramen (free edge of the lesser omentum) indicated by the arrow, which identifies the portal triad within that boundary?
What is the column of Bertin in the kidney?
Which anatomical lobe of the liver is the caudate lobe?
Which part of the gastrointestinal tract is anatomically associated with 'appendices epiploicae'?
What is the relation of the caudate lobe of the liver?
Couinaud's segments are used to divide which organ?
Which of the following organs does not have a portosystemic shunt?
A 45-year-old male presented with severe abdominal pain. His cremasteric reflex was noted to be absent during physical examination. Which of the following nerves is responsible for the efferent limb of the cremasteric reflex?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app