
Abdomen — MCQs

On this page
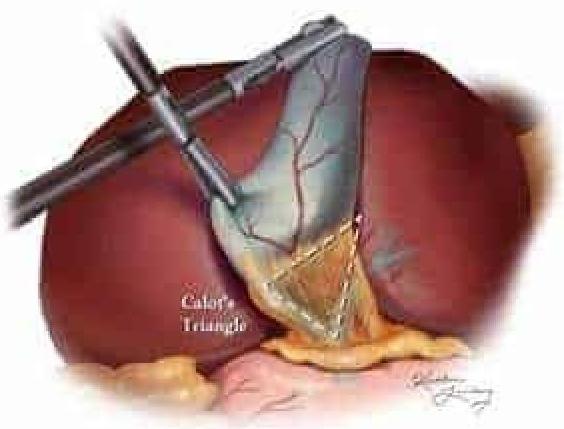
Which of the following structures is not a boundary of Calot's triangle shown in the given image?
Cholecystocaval line separates:
What is the shape of caecum in the newborn?
Which of the following statements about the bare area of the liver is false?
Which of the following structures does NOT pass through Calot's triangle?
Spleniculi are most commonly found in which of the following locations?
Sensory nerve supply of gall bladder is through -
Inferior epigastric artery forms the boundary of?
Which of the following is not formed by the external oblique muscle?
Which of the following is NOT a boundary of the foramen of Winslow?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app