
Abdomen — MCQs

On this page
A 55-year-old man complains of anorexia, weight loss, and fatigue. A UGI study demonstrates an ulcerated lesion at the incisura. Where is the incisura?
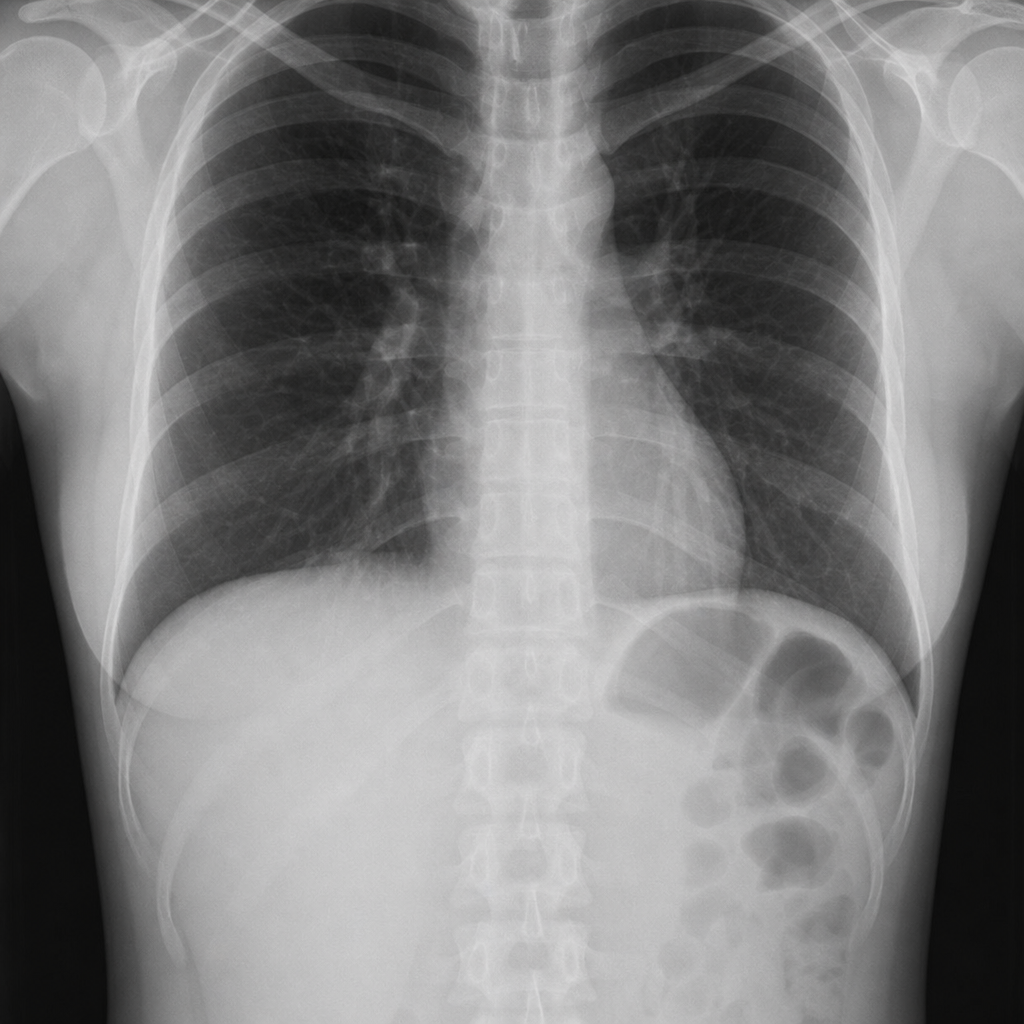
A 28-year-old female presents for a physical examination for an insurance policy. Physical and laboratory examinations suggest she is a normal, healthy woman. An abdominal radiograph of the patient is shown below, demonstrating a tongue-like caudal projection from the inferior margin of the right lobe of the liver. Which of the following is the most likely diagnosis?
All of the following are anterior branches of the abdominal aorta except?
The splenic artery is a branch of which of the following arteries?
The neck of the sac of a femoral hernia lies at which anatomical position relative to the pubic tubercle?
Which of the following is NOT a normal feature of the colon?
A 58-year-old male alcoholic is admitted to the hospital after vomiting dark red blood (hematemesis). Endoscopy reveals ruptured esophageal varices, resulting from portal hypertension. Which of the following venous tributaries to the portal system anastomoses with caval veins to cause the varices?
All of the following are true about the caudate lobe except?
The nerve of Grassi is anatomically related to which of the following nerves?
A young athlete, after rigorous training and strict diet control, develops a 'washboard stomach'. Which of the following structures marks its lateral border?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app