
Abdomen — MCQs

On this page
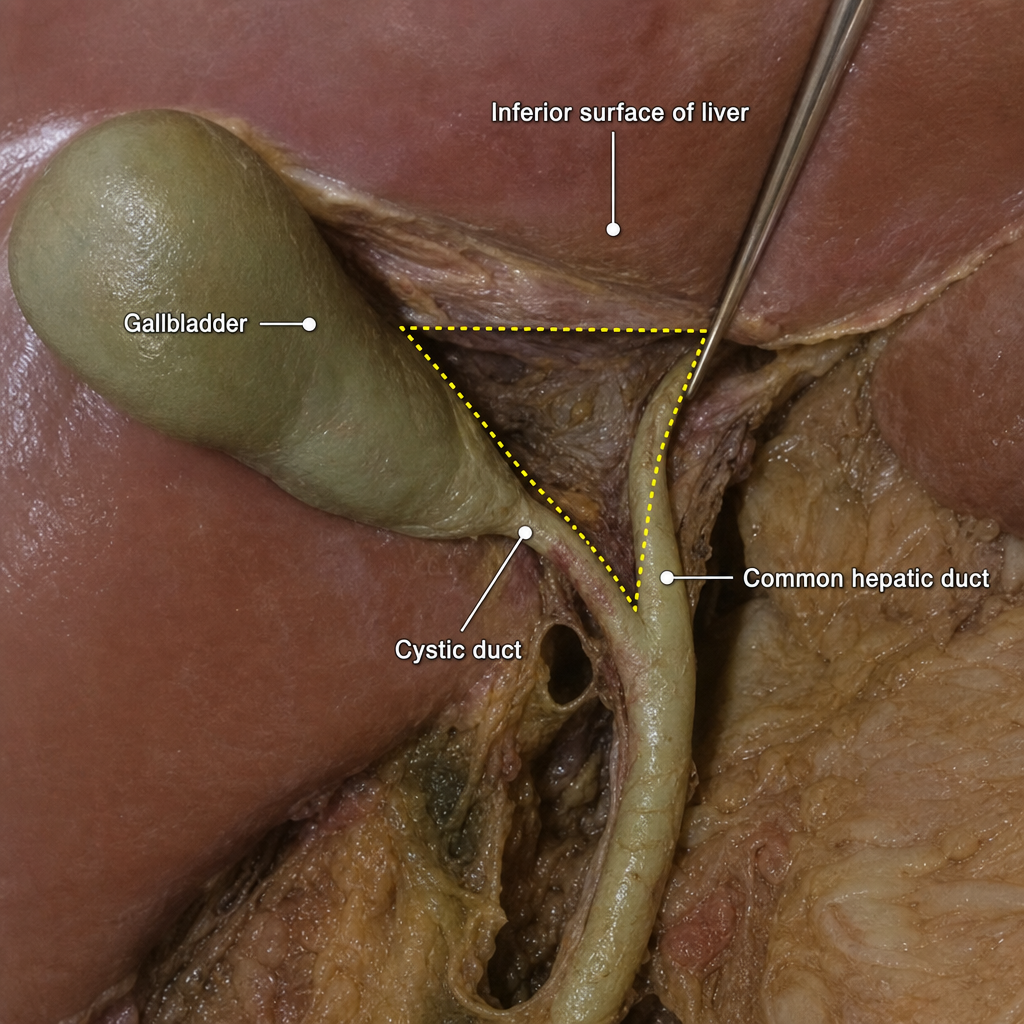
Which of the following structures is NOT a boundary of the hepatocystic triangle?
The gallstone pain is referred to the shoulder through which of the following nerves?
The squamo-columnar junction is normally located at
Which of the following statements about the caudate lobe of the liver is true?
How many layers does the greater omentum have?
Which artery primarily supplies the stomach?
The majority of gastric lymph ultimately drains to which of the following?
In posterior perforation of stomach, collection of gastric contents occurs in which pouch?
Which segment of the liver receives blood supply from both the right and left hepatic arteries and portal veins, and drains directly into the inferior vena cava?
To which segment of the liver is the gallbladder related?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app