
Abdomen — MCQs

On this page
To which lymph nodes, the lymph from the umbilicus drain?
Which of the following ligaments contains splenic artery?
The pancreas is supplied by all of the following arteries except
The transition between the stomach and duodenum is marked by
Normal anatomical narrowings of the ureter are present in all EXCEPT:
Which one of the following statements regarding Cantlie's line is correct?
Which of the statements regarding Calot's triangle are correct? 1. Common hepatic duct forms the medial boundary of the Calot's triangle 2. Inferior surface of the right lobe of the liver forms the superior boundary of Calot's triangle 3. Right hepatic artery is usually found as a content of the Calot's triangle 4. Cystic duct and medial border of gall bladder forms the lateral border of Calot's triangle Select the correct answer using the code given below:
In the intraoperative image of congenital hernia repair, the structure marked by the red arrow is identified as which of the following?
Anterior relations of third part of duodenum are all except?
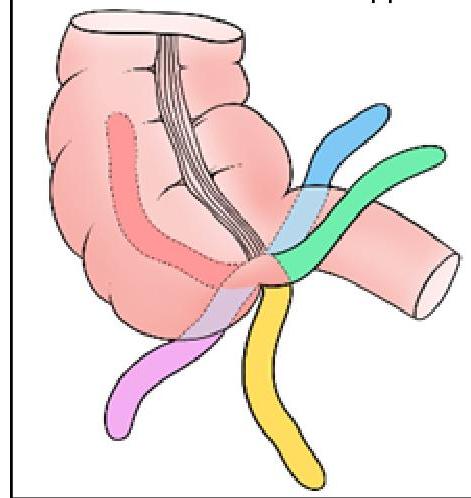
Identify the position of the appendix marked in BLACK in the given image:
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app