
Abdomen — MCQs

On this page
Which of the nerves shown in yellow color is not a part of the triangle of pain?
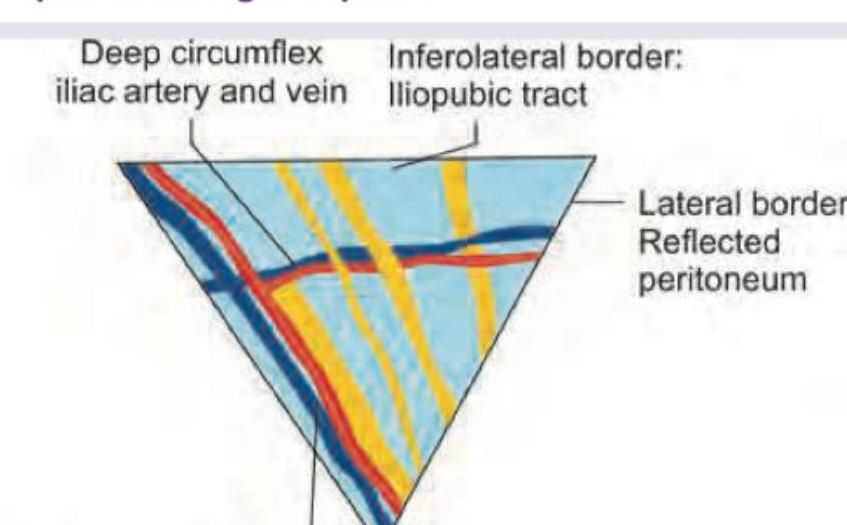
Identify the nerve passing through the Triangle of Doom:
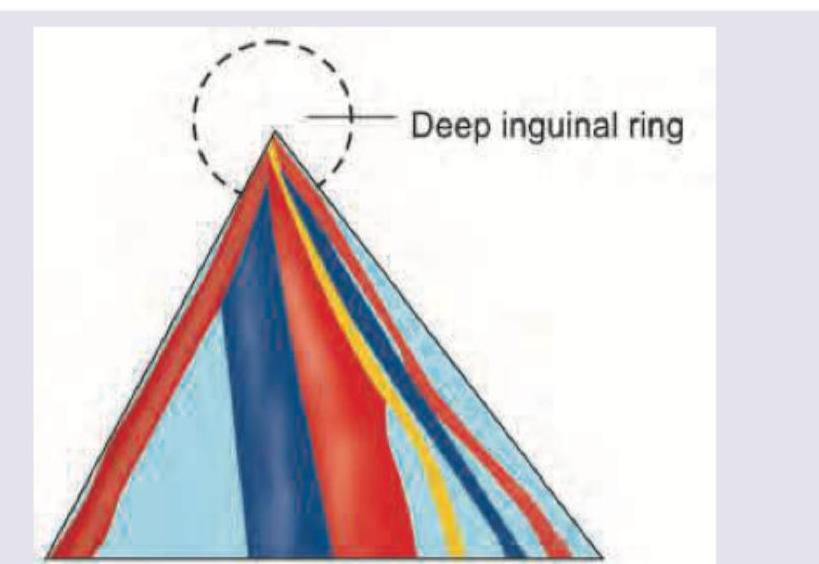
Which of the following marks the conjoint tendon?
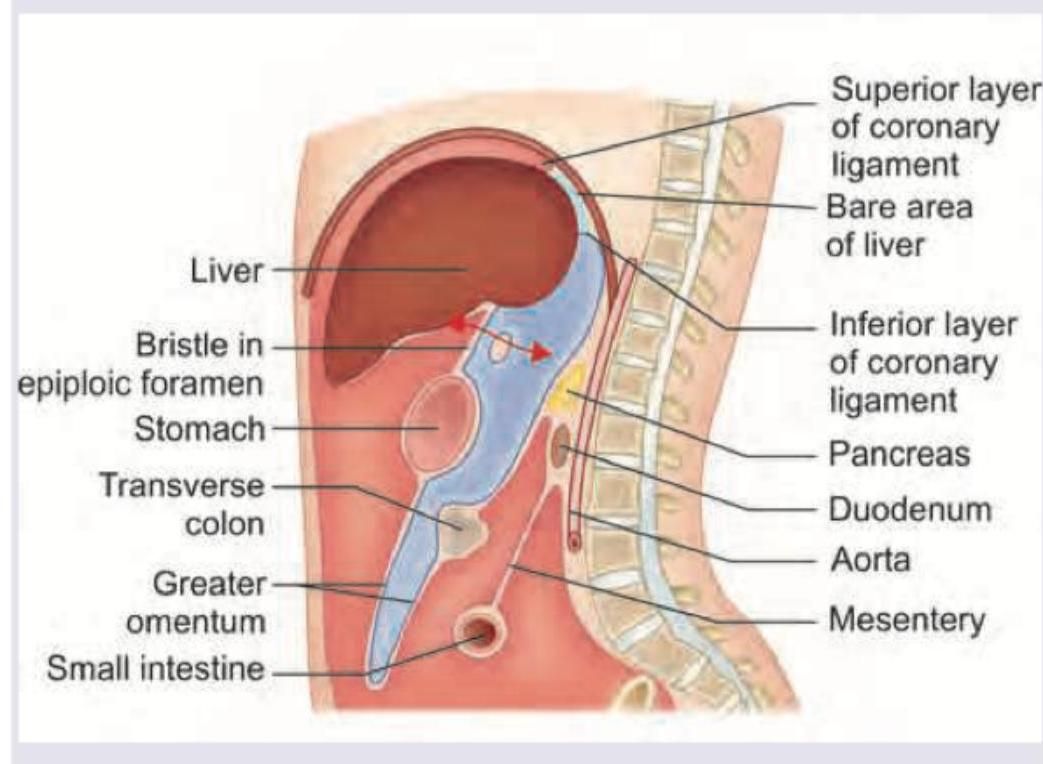
Identify the structure that forms the superior border of the epiploic foramen (marked in red) in the image below.
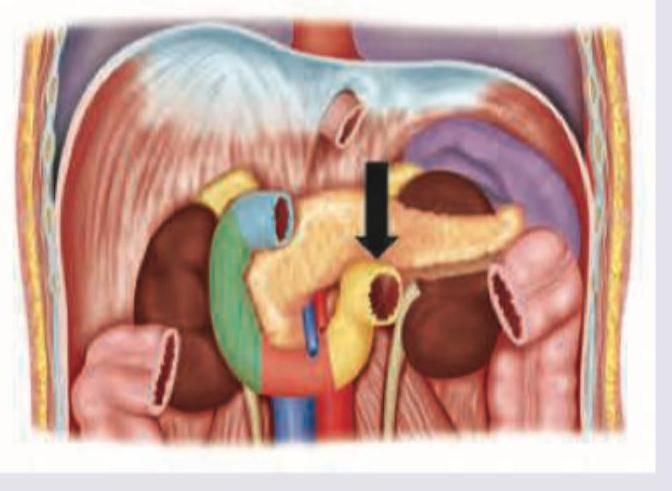
Identify the part of the duodenum marked below:
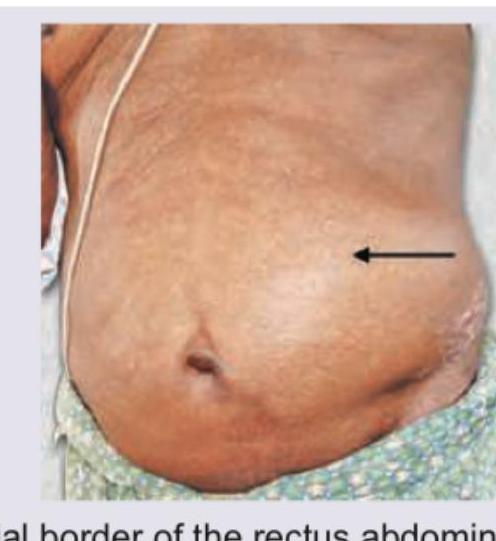
Hernia that is depicted in the image usually occurs at:
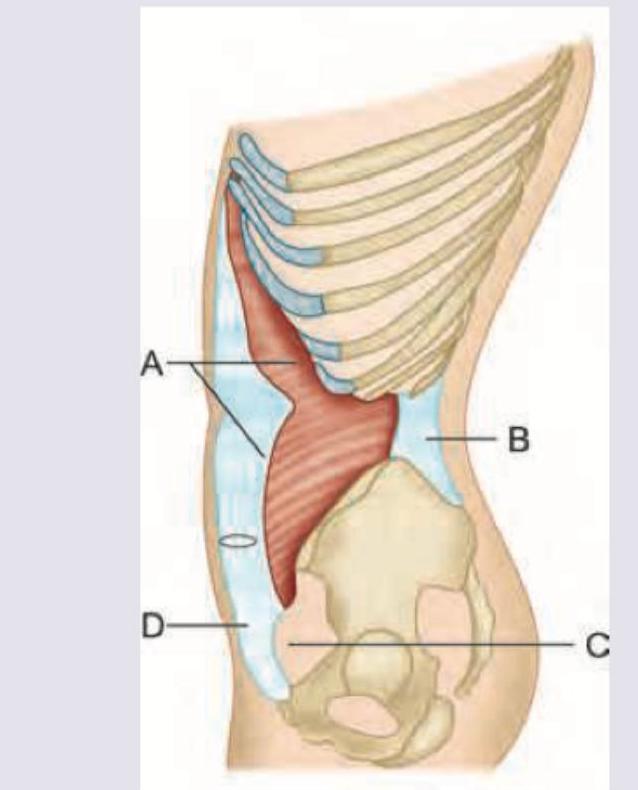
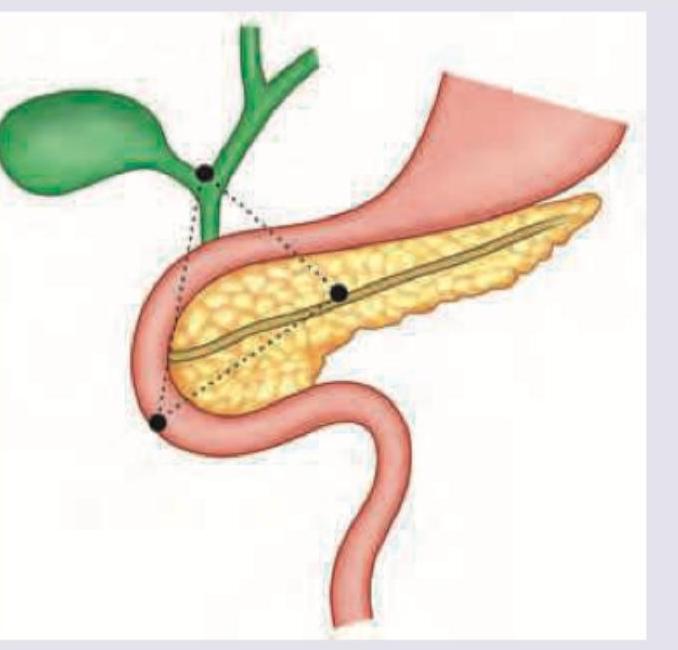
Which triangle is shown here?
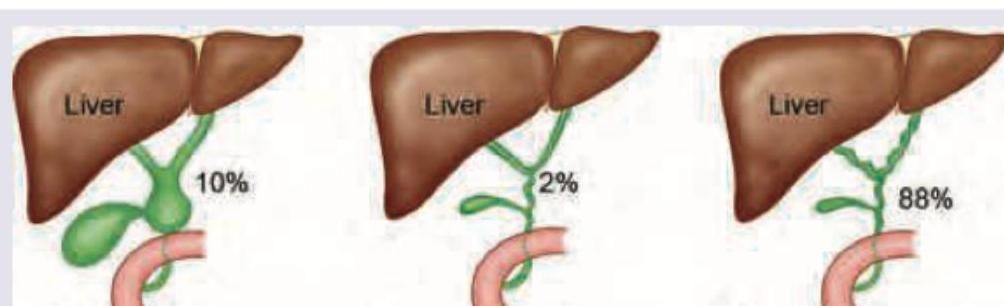
Which of the following is the most common variety of biliary tree: (Recent NEET Pattern 2016-17)
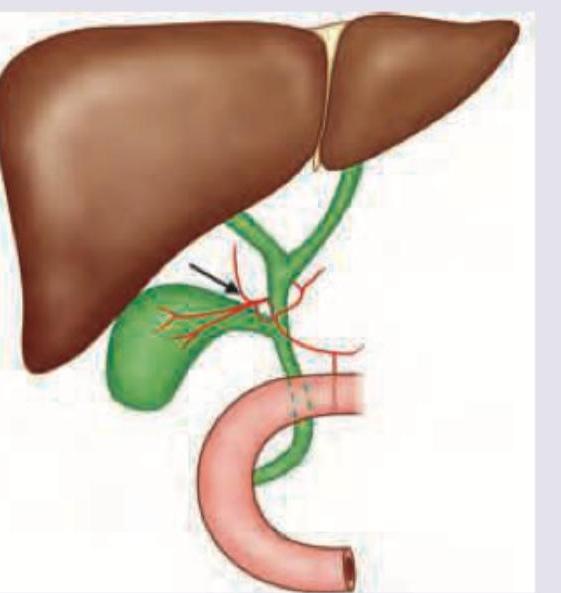
The following arrow marked vessel can cause torrential hemorrhage during cholecystectomy. Which of the following is the correct description?
All are true about the reflex being elicited except?

Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app