
Abdomen — MCQs

On this page
Which of the following blood vessels is Drummond's Artery? (Recent NEET Pattern 2016-17)
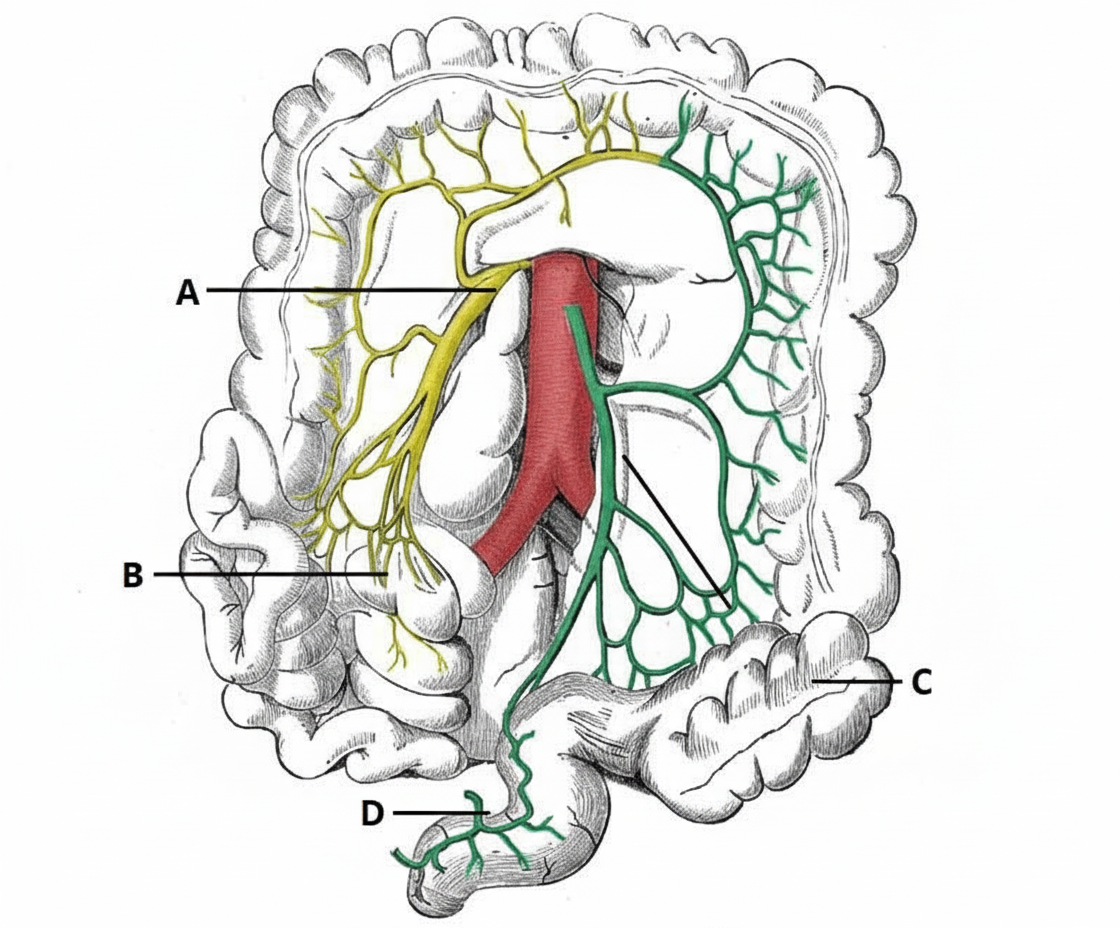
Which of the following blood vessels is present in the peritoneal reflection of the paraduodenal fossa?
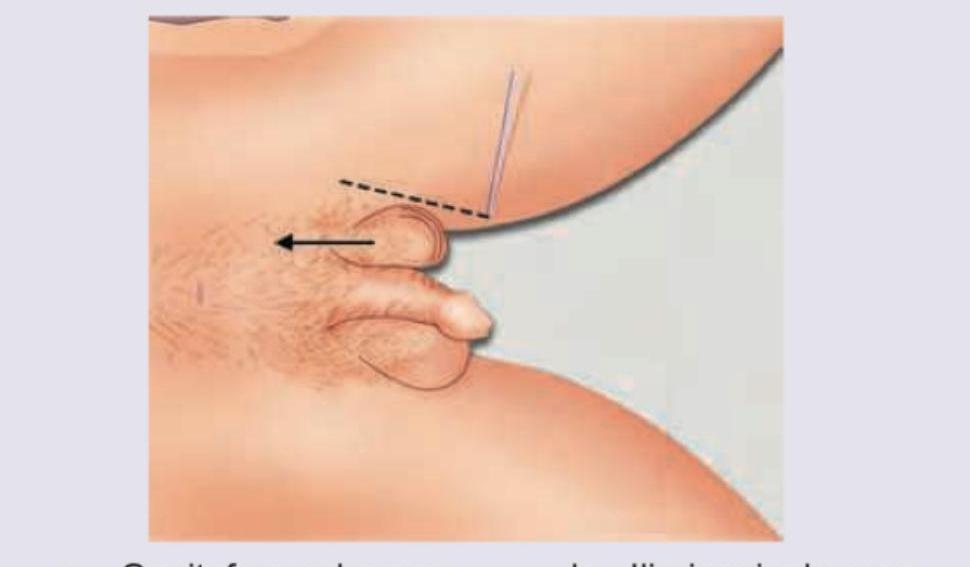
What is the afferent nerve of the superficial reflex shown?
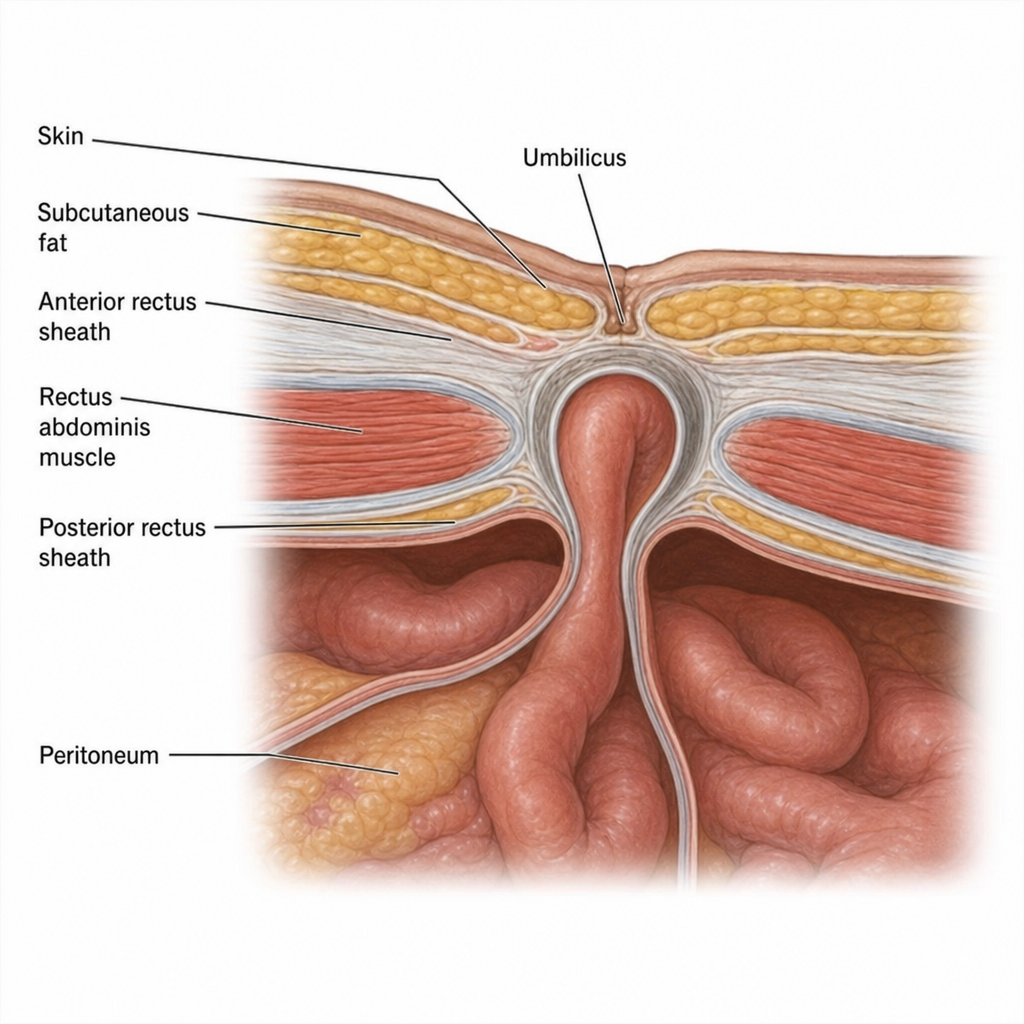
Which of the following hernia is shown in the following representation? (Recent NEET Pattern 2016-17)
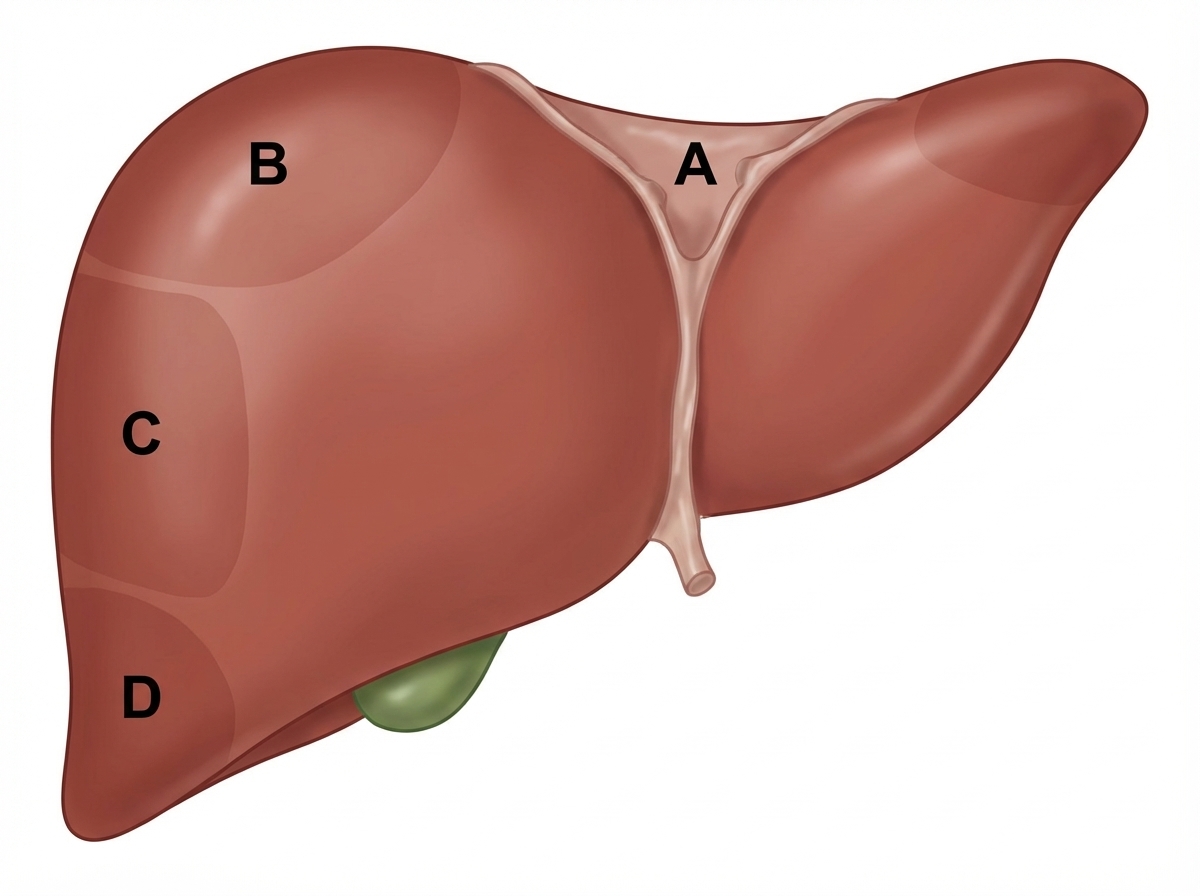
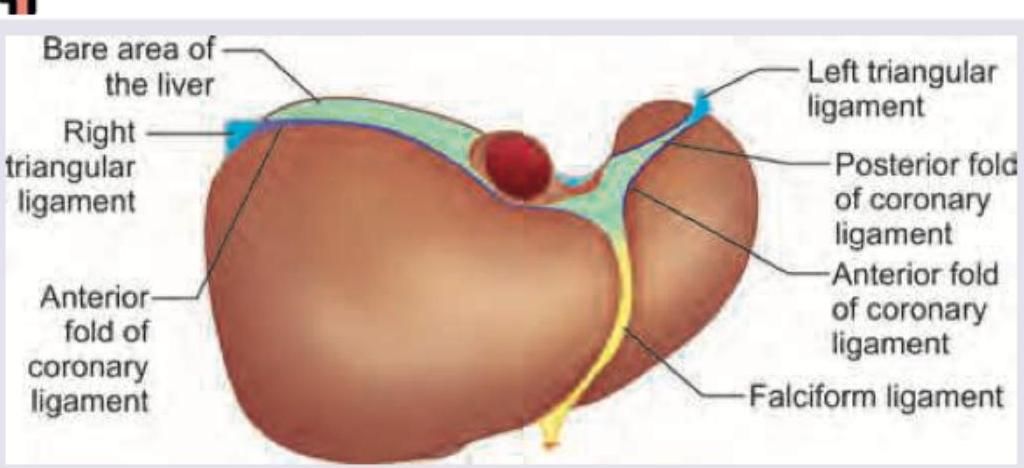
Which of the following is the bare area of liver?
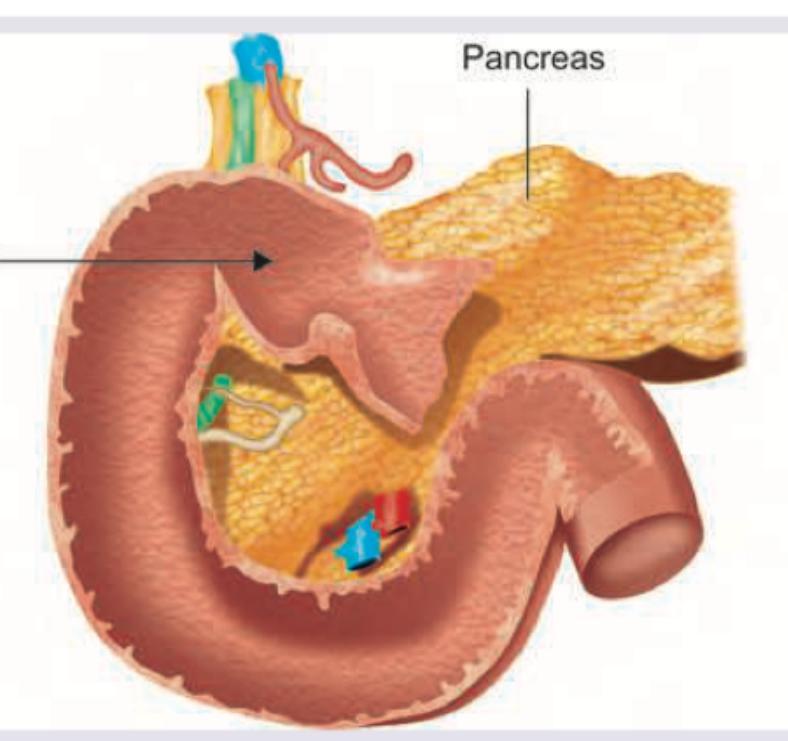
All of the following are correct about the part of duodenum marked as 1 except?
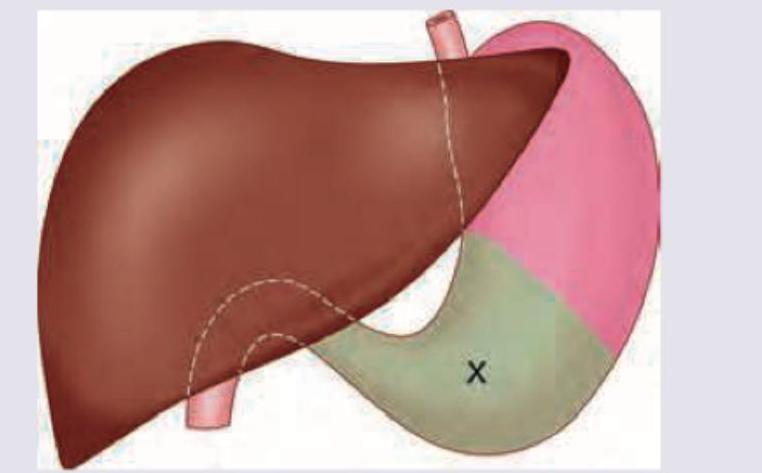
The area marked as $X$ was selected for gastrostomy. Which of the following statements is incorrect about this area? (Recent NEET Pattern 2016-17)
Name the structure marked as $X$?
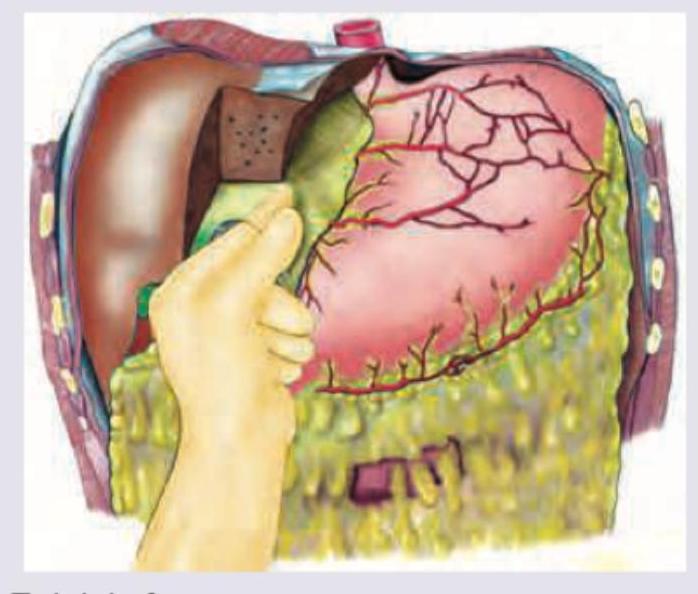
All are true about the site where the gloved hand of the surgeon is located except?
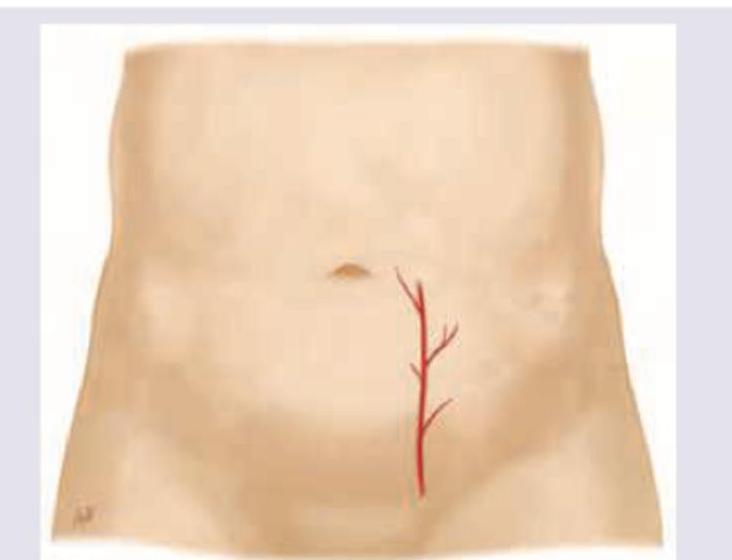
Which artery shown here should be avoided during paracentesis?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app