
Abdomen — MCQs

On this page
A 55-year-old man is diagnosed with left testicular carcinoma. Which of the following lymph nodes is the first to be involved?
The ligament of Treitz (suspensory ligament of the duodenum) marks the anatomical boundary between which two structures?
Which of the following is not a boundary of the hepatocystic triangle?
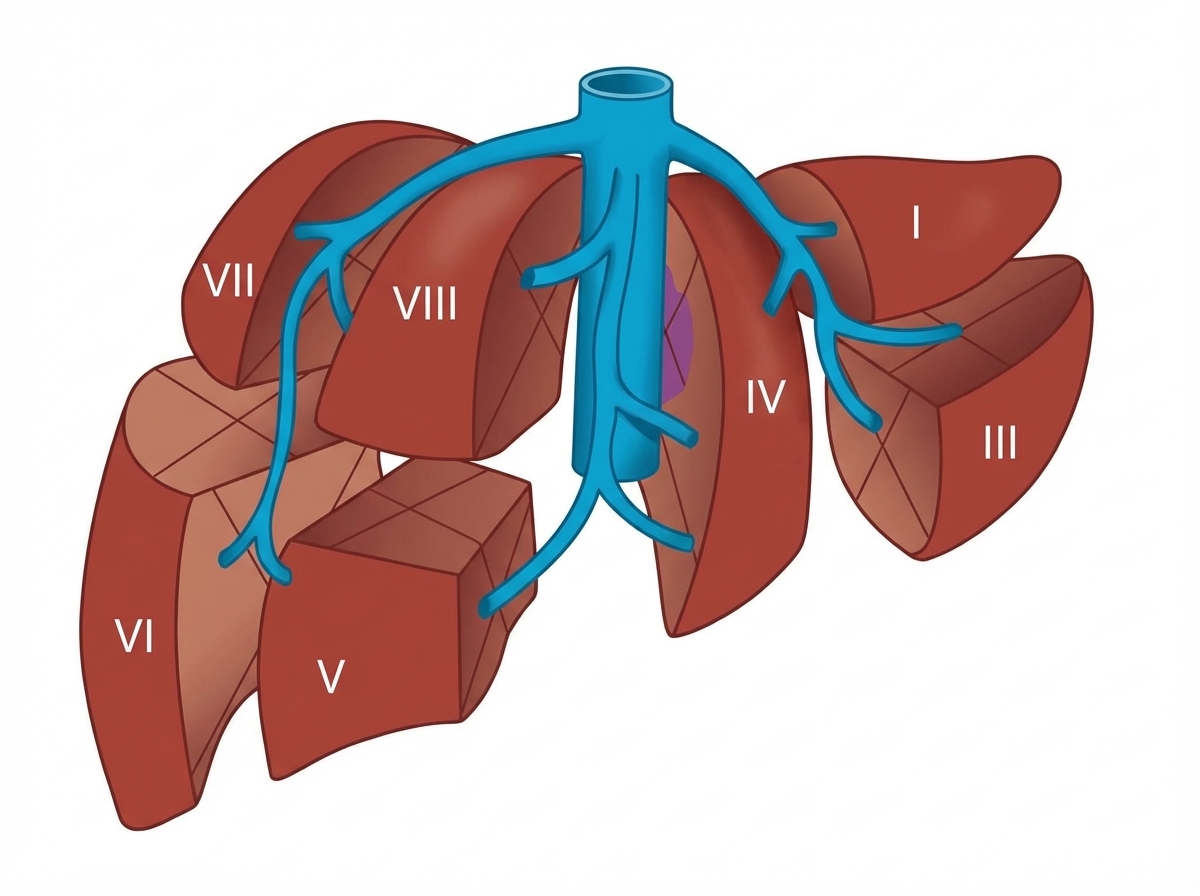
The image shows which anatomical classification system?
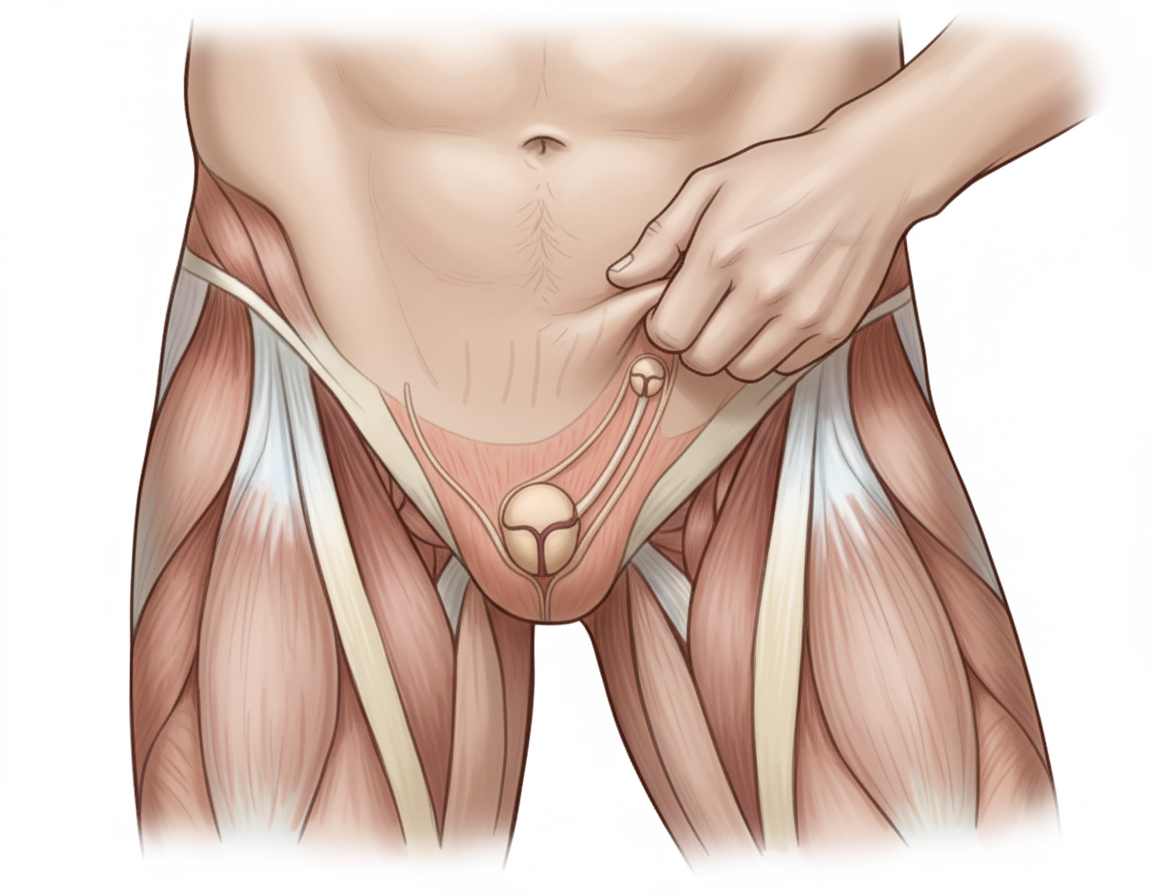
The image shows performance of the Cremasteric Reflex with ipsilateral elevation of testis. Which nerve mediates this reflex? Additional information: - Afferent: Femoral branch of genitofemoral nerve - Efferent: Genital branch of genitofemoral nerve - The reflex is elicited by lightly stroking the skin on the medial aspect of the superior part of the thigh - Rapid elevation of the testis on the same side confirms the cremasteric reflex - This reflex is extremely active in children
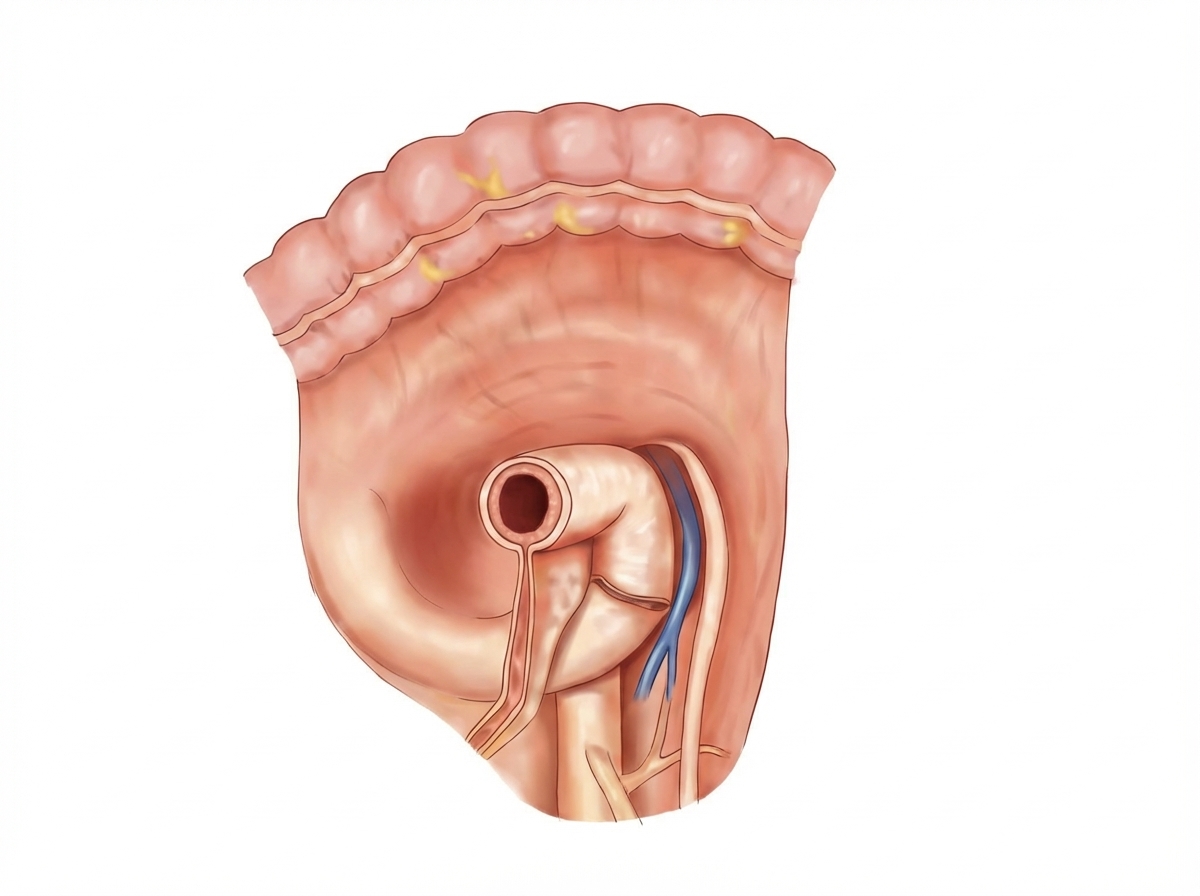
The image shows the para-duodenal fossa region. The para-duodenal fossa is a sickle-shaped fold of peritoneum, sometimes found arching between the left side of the duodeno-jejunal flexure and the medial border of the left kidney. Its right free edge forms the anterior boundary of the para-duodenal recess. Which structure is contained in the right free edge of the para-duodenal fold?
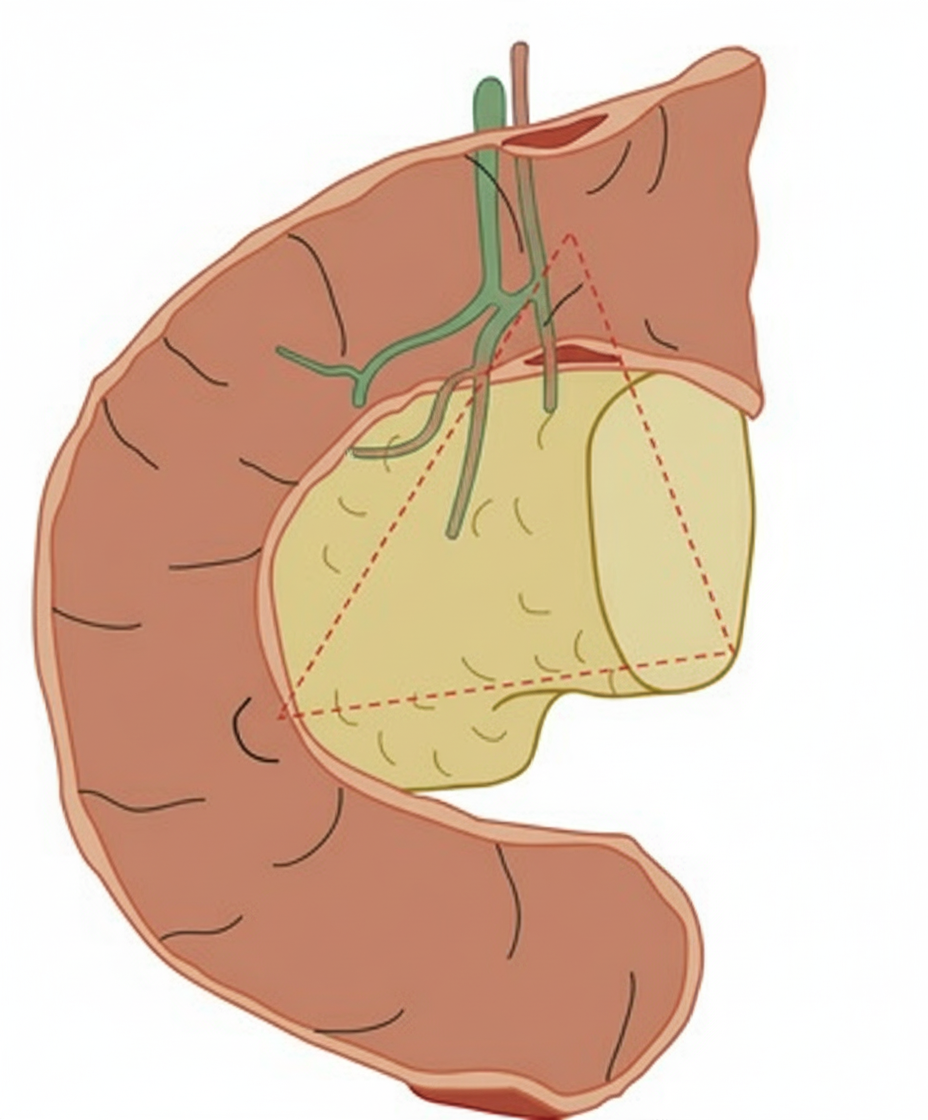
The image shows a triangular anatomical region with the following boundaries: 1. Confluence of cystic duct with common hepatic duct 2. Junction of head and body of pancreas 3. Junction of second and third parts of duodenum. Identify the structure:
Identify the structure indicated by the pointer in the image.
The structure marked X on the image below is:

The following image of posterior abdominal wall and pelvic inlet shows a structure marked as X. Identify it:

Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app