
Abdomen — MCQs

On this page
The Couinaud's segmental nomenclature is based on the position of which vascular structures?
Which of the following statements is NOT true about the right kidney?
Which of the following is NOT a content of the rectus sheath?
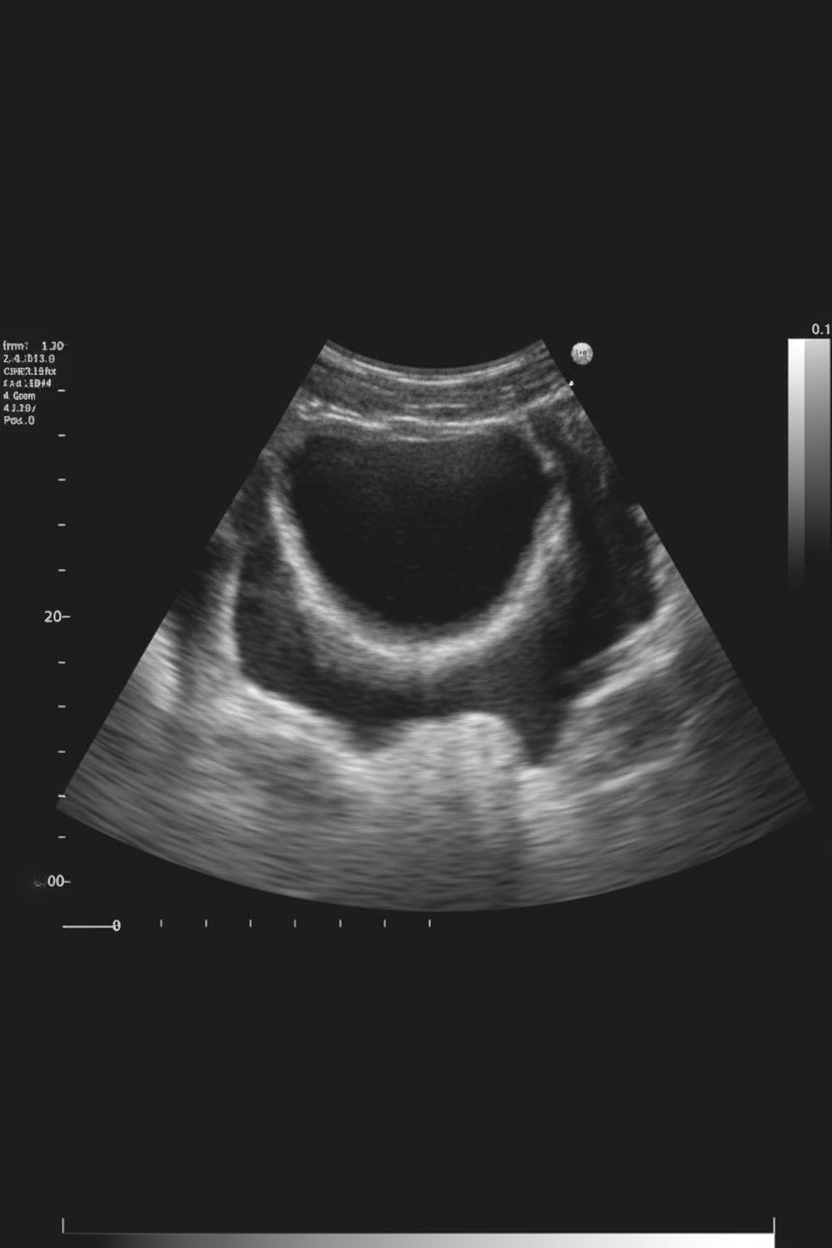
The congenital anomaly of the gallbladder shown in the image is:
The left ureter is related to which of the following structures?
The second part of the duodenum is not related posteriorly to which of the following structures?
Pain in the hypogastric region may arise from which of the following organs?
Which of the following is NOT a basis for the division of anatomical segments of the liver?
What is the approximate length of the ureter?
Which of the following is WRONG about the ileum when compared with the jejunum?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app