
Abdomen — MCQs

On this page
During an abdominal surgical procedure, the surgeon wishes to locate the ureter in order to ensure that it is not injured. The ureter may be found immediately anterior to the origin of the?
What is the posterior relation of the epiploic foramen?
Which of the following is NOT found in the Space of Disse?
A 42-year-old obese woman with seven children is brought to a local hospital by her daughter. Physical examination and her radiograph reveal that large gallstones have ulcerated through the posterior wall of the fundus of the gallbladder into the intestine. Which of the following parts of the intestine is most likely to initially contain gallstones?
Which of the following accurately describes a boundary of the lesser sac (omental bursa)?
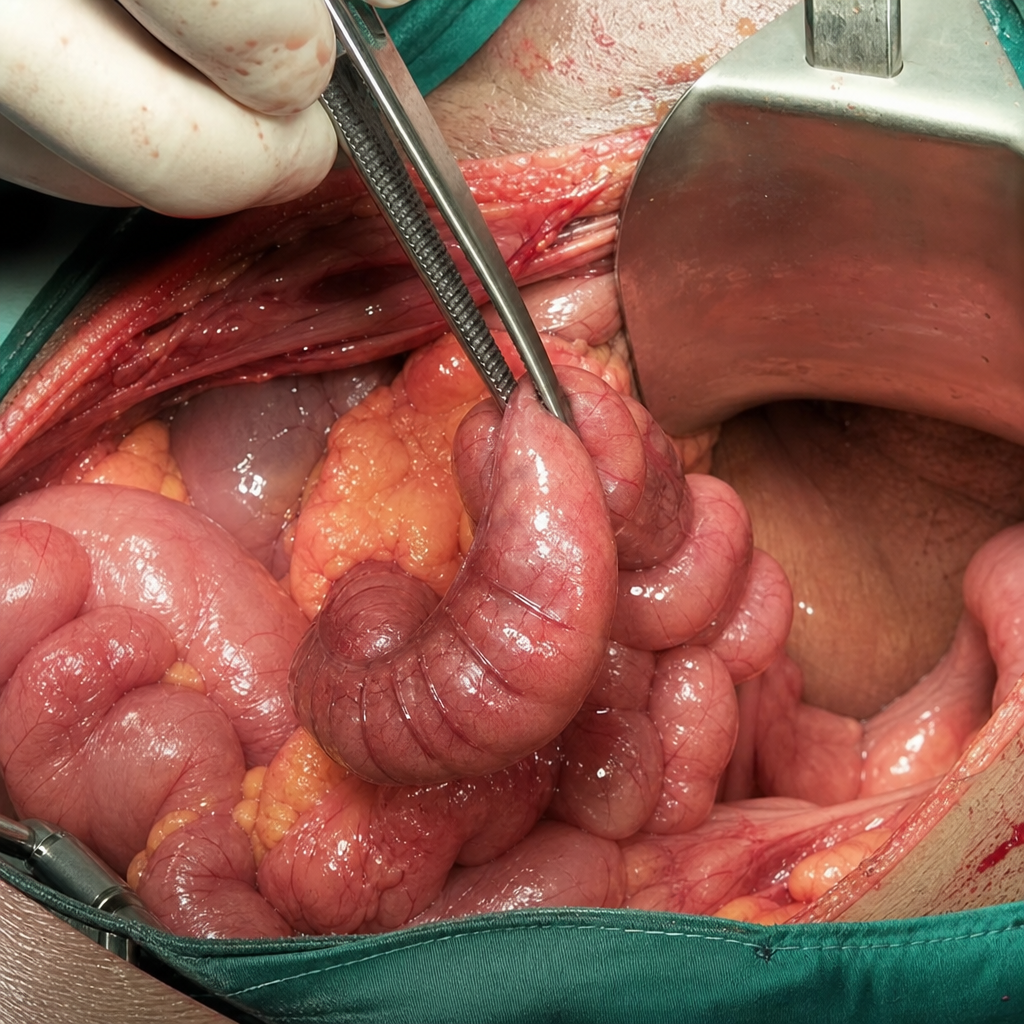
Which structure is held by forceps?
Portocaval anastomosis is seen at all of the following locations, except?
The portal vein is related to all of the following structures except:
Which of the following is an anterior peritoneal relation of the right kidney?
A patient is admitted from the emergency department following a large-volume haematemesis. Oesophagogastroduodenoscopy is performed, which identifies a posteriorly positioned duodenal ulcer that is actively bleeding. What is the vessel responsible for this bleeding?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app