
Abdomen — MCQs

On this page
Which location of a renal stone is most likely to cause pain radiating to the medial side of the thigh and perineum in males due to the stone slipping?
The left gastric artery is a branch of which of the following?
A 27-year-old woman has suffered a gunshot wound to her mid abdomen. After examining the patient's angiogram, a trauma surgeon locates the source of bleeding from pairs of veins that typically terminate in the same vein. Which of the following veins are damaged?
Ureteric constructions are seen at all the following positions, EXCEPT:
While exposing the kidney from behind, which of the following nerves is least likely to be injured?
Surgical lobes of the liver are divided on the basis of which of the following structures?
A 50-year-old male, a known case of diverticulosis of the colon, presents with complaints of left lower quadrant pain and bloody stools. He is scheduled for follow-up. The physician begins the workup with an appropriate test of the sigmoid colon by recalling which of its specific features?
A 43-year-old woman is admitted to the emergency department with esophageal pain and hematemesis after swallowing a fish bone. An endoscopic examination reveals perforation of the intraabdominal portion of the esophageal wall. Which of the following arteries is most likely injured?
Which of the following statements is TRUE about the Lumbar plexus?
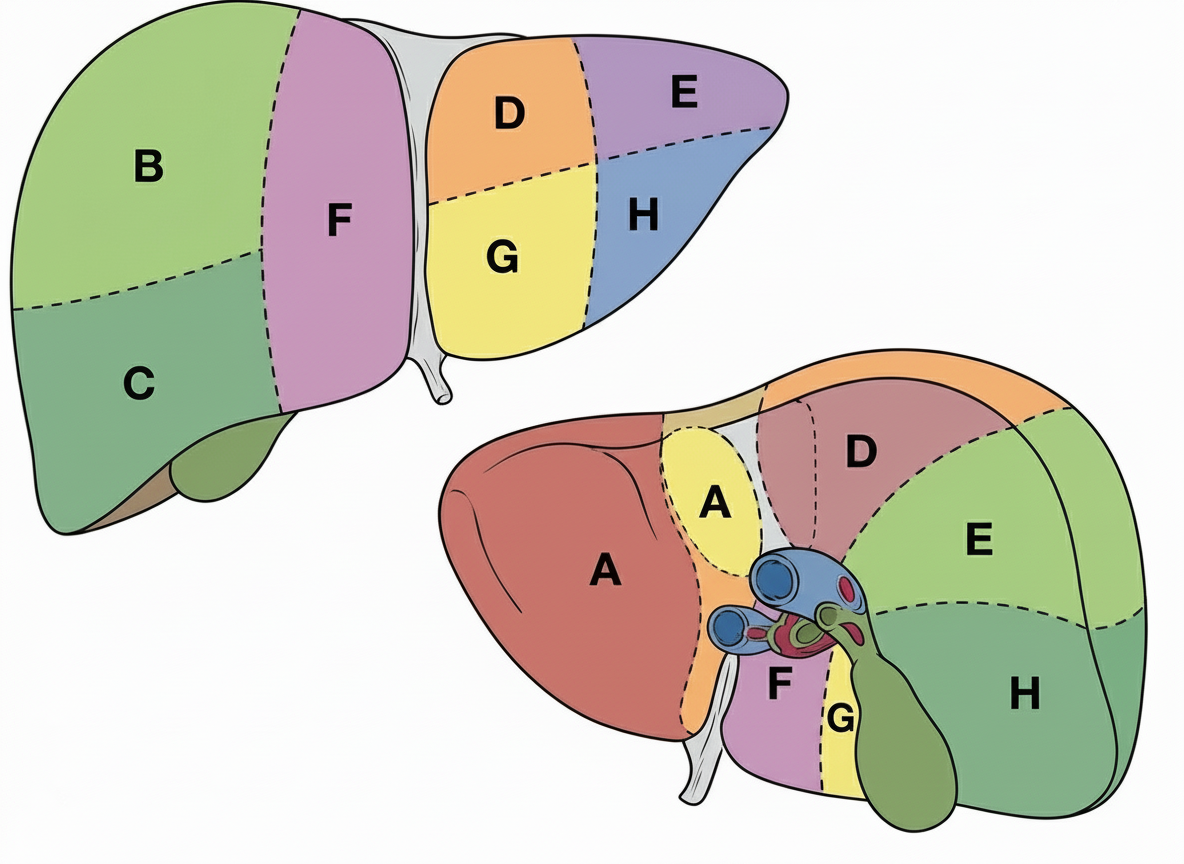
Identify the liver segment marked 'F' as per Couinaud's classification?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app