
Abdomen — MCQs

On this page
What is an epicolic lymph node?
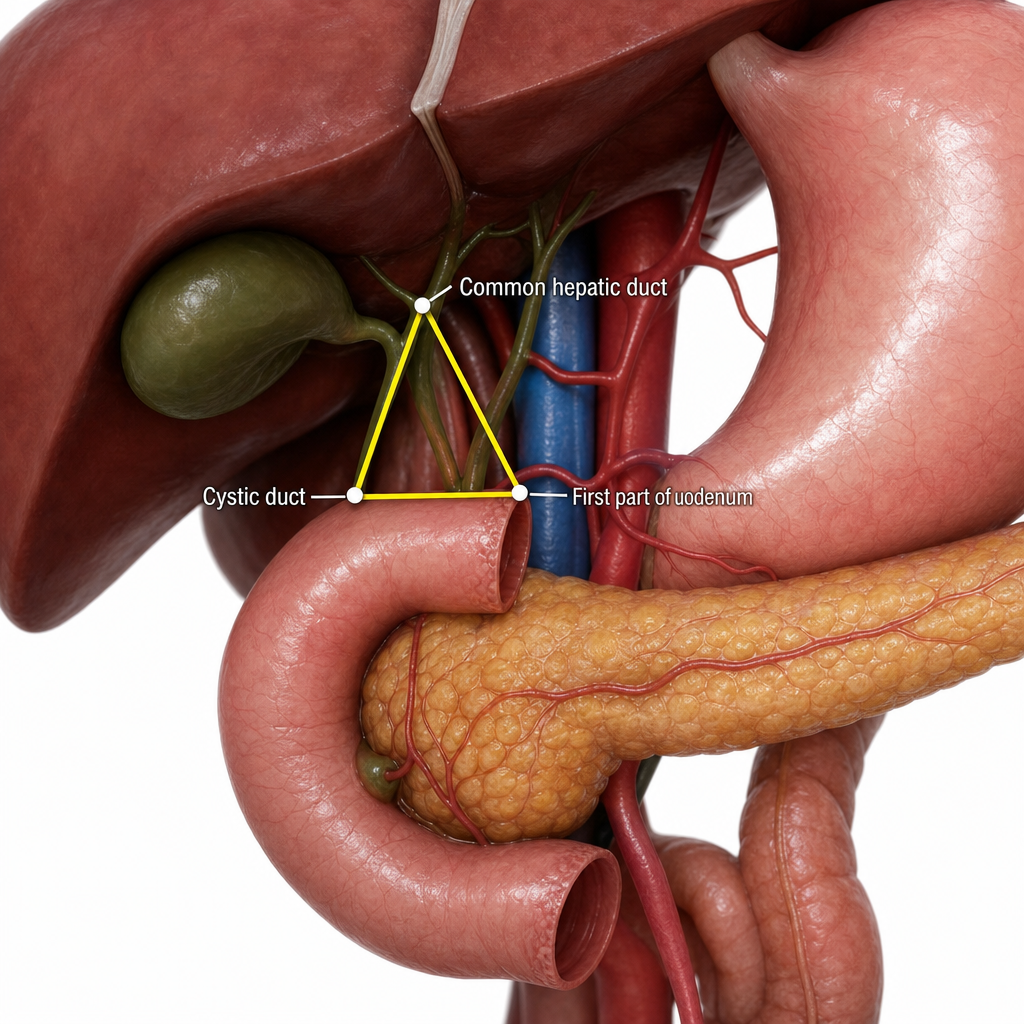
Which anatomical triangle is described by the given image?
The Sphincter of Lutkens is found in which anatomical structure?
Regarding the blood supply of the pancreas, which of the following statements is true?
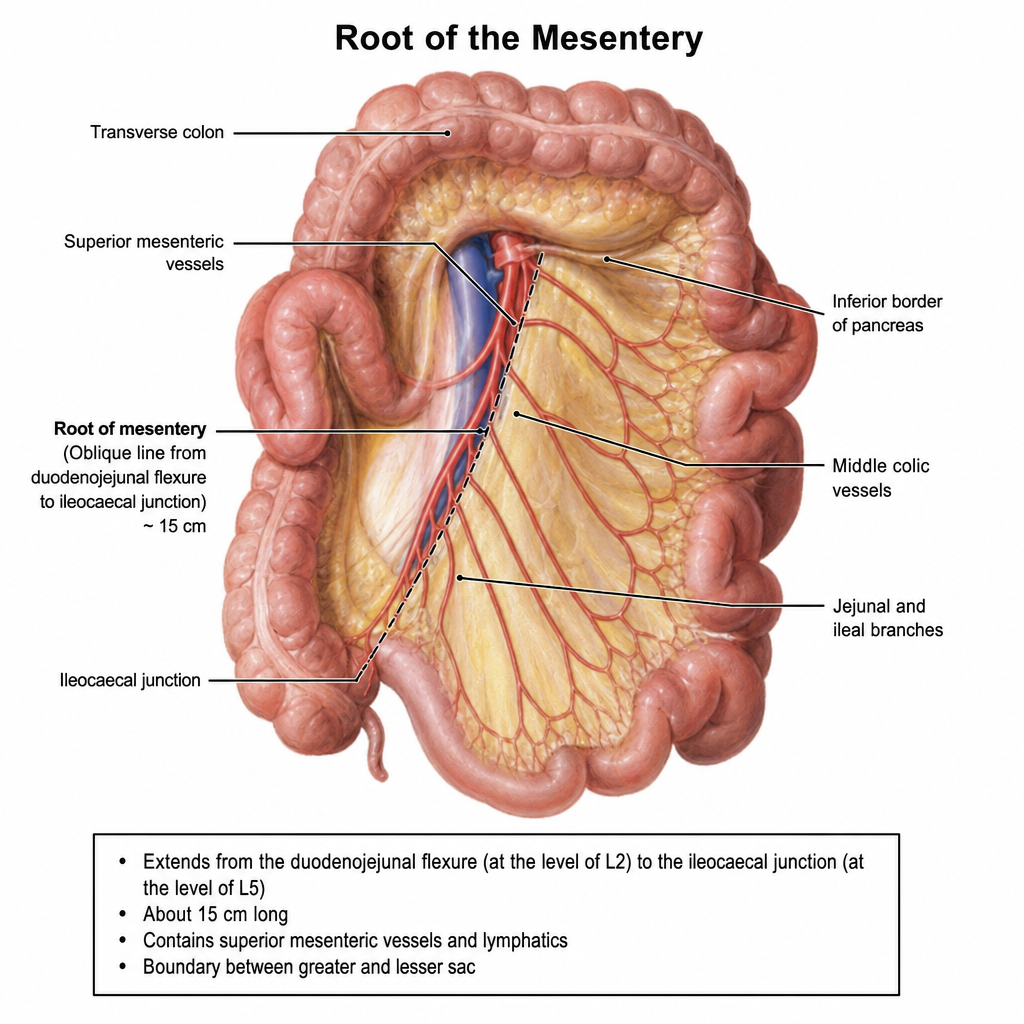
Which of the following statements regarding the root of the mesentery are false? **Statement 1:** The root of the mesentery begins at the duodenojejunal flexure, which is located to the right of the L2 vertebra. **Statement 2:** The root of the mesentery ends at the ileocaecal junction at the level of the right sacroiliac joint. **Statement 3:** The root of the mesentery crosses the 2nd (descending) part of the duodenum. **Statement 4:** The root of the mesentery passes obliquely downwards and to the right.
At which vertebral level does the portal vein originate?
The transpyloric plane passes through which structure?
What lies between the cystic duct and the common hepatic duct?
The spleen is supplied by all of the following except:
The inferior mesenteric artery supplies all of the following except?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app