
Abdomen — MCQs

On this page
In portal hypertension, which of the following is NOT a site of portosystemic anastomosis?
The duodenum lies at which of the following vertebral levels?
Which location of a renal stone is most likely to cause pain radiating to the medial side of the thigh and perineum in males?
What is true about the inferior vena cava?
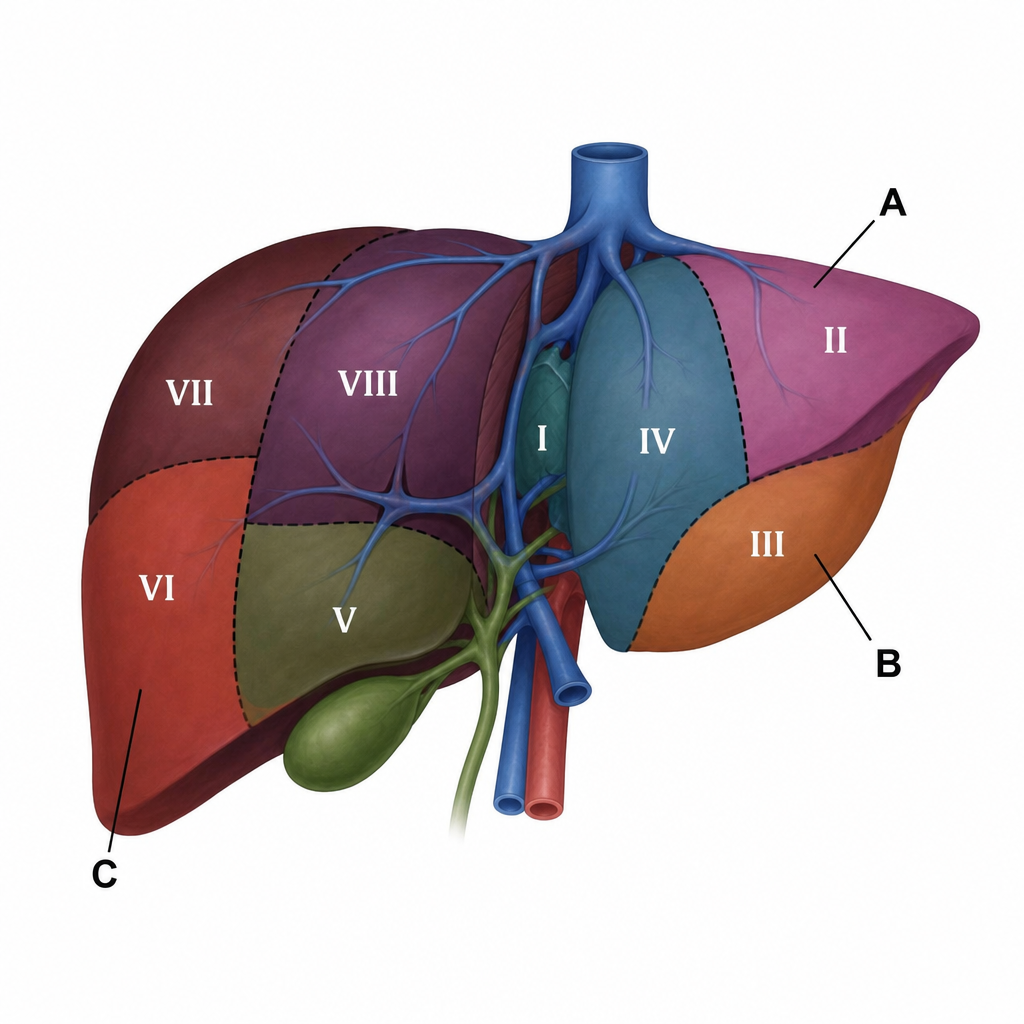
Which of the following marked structures represents the 9th segment of the liver?
Compression of the inferior mesenteric vein just before it joins the splenic vein would most likely result in enlargement of which of the following veins?
Cremasteric artery is a branch of which artery?
What is true about the inguinal canal?
Which of the following is NOT included in the lymphatic drainage of the stomach?
Which of the following structures is possessed by the appendix?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app