
Abdomen — MCQs

On this page
Which statement best completes this sentence: The superior mesenteric artery:
Varicocele is common on the left testis because?
In attempting to minimize complications during cholecystectomy, the surgeon defines the triangle of Calot. The boundaries of the triangle of Calot (modified) are the common hepatic duct medially, the cystic duct inferiorly, and the liver superiorly. Which structure courses through this triangle?
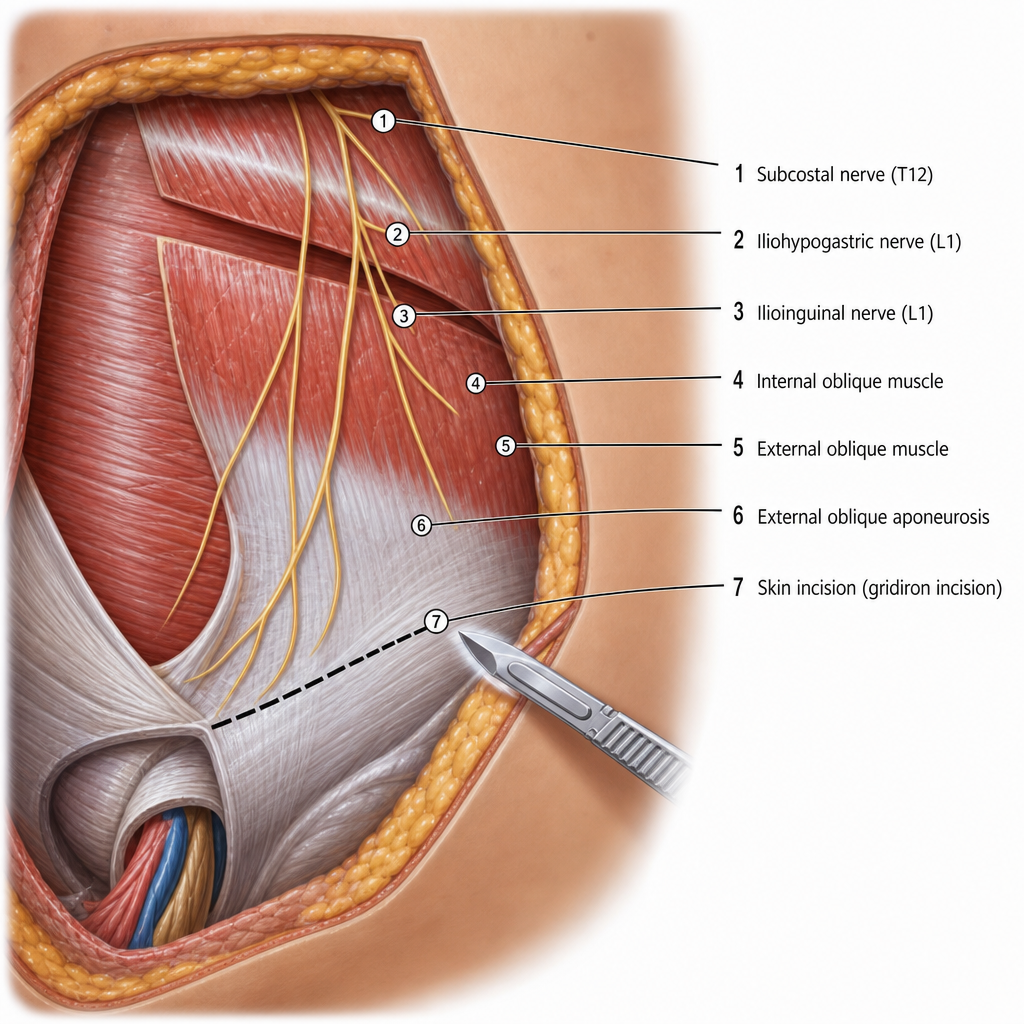
Which nerve is most commonly injured in the depicted incision?
Which statement best completes this sentence? The porta hepatis contains:
The ureter lies against the anterior surface of which of the following muscles?
Which organ has dual blood supply?
The cisterna chyli are situated in which of the following regions?
What is the most common site of ischemia of the large bowel?
What is the nerve supply to the skin around the umbilicus?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app