
Abdomen — MCQs

On this page
Which of the following statements is NOT true regarding the common bile duct?
In a left loin nephrectomy, which muscle is NOT cut?
Commonest location of Spigelian hernia is at which anatomical region?
A tumor of the uncinate process of the pancreas affects which of the following vessels?
Which vessel is at risk during a Maylard incision on the anterior abdominal wall?
Which membrane is encountered when attempting to reach the lesser peritoneal sac and the head of the pancreas after penetrating the greater peritoneal sac?
A patient presents with pain in the right testis. Examination reveals a 'bag of worms' appearance, suggestive of a varicocele. Into which vessel does the right testicular vein drain?
A 41-year-old man presented with abdominal pain two months postoperatively following emergent surgery for abdominal trauma. A CT scan demonstrated an internal hernia involving the hepatic flexure of the colon herniated through the epiploic foramen. Gastrointestinal veins appeared markedly dilated, including veins forming anastomoses between the portal and caval systems. Which of the following structures is most likely compressed?
A 29-year-old man presents with duodenal peptic ulcer and complains of cramping epigastric pain. Which of the following structures harbors the cell bodies of abdominal pain fibers?
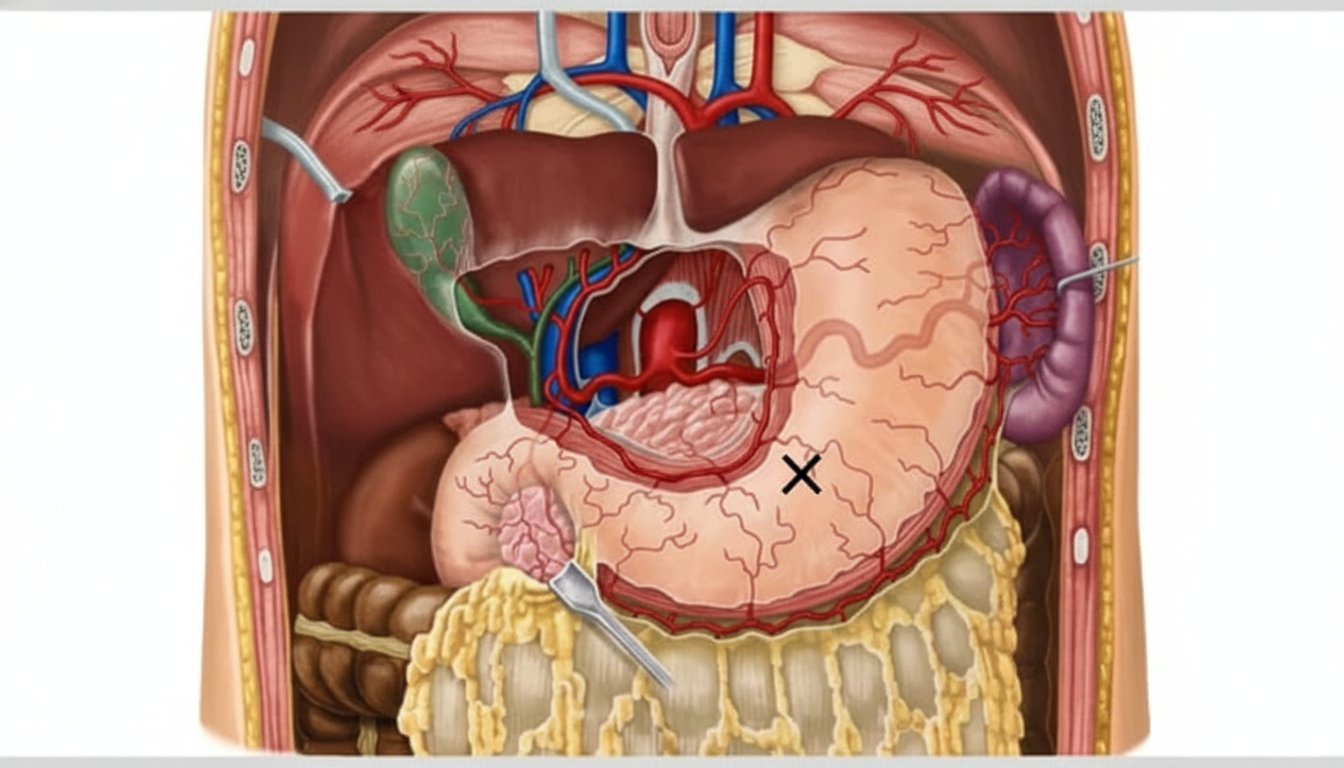
The artery marked X is most commonly a branch of?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app