
Abdomen — MCQs

On this page
Which of the following statements is true regarding the anatomical relationships of the renal artery and vein?
The paraduodenal recess is anatomically associated with which major vessel?
What is the shortest part of the colon?
A 49-year-old woman presents with abdominal pain. Physical examination reveals epigastric pain that radiates toward the right side and posteriorly toward the scapula. Radiographic examination shows cholecystitis with a large gallstone and no jaundice. In which of the following structures is the gallstone most likely located?
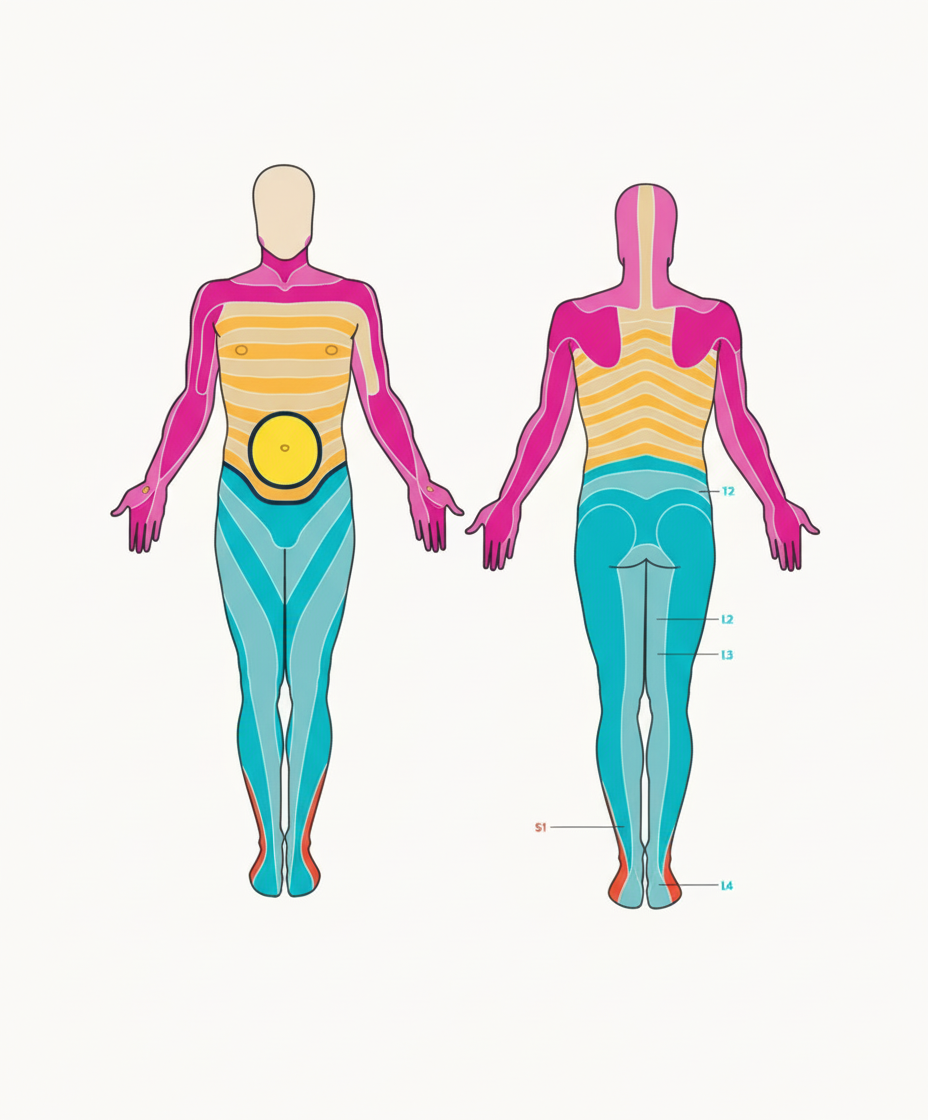
A patient presented with midline periumbilical pain at the marked dermatome, associated with nausea and a low-grade fever. There are no urinary symptoms and no flank tenderness. Which of the following is the most likely differential diagnosis?
Where is the spiral valve seen?
A 62-year-old woman presents with abdominal pain of uncertain origin. A CT scan reveals an aortic aneurysm at the origin of the superior mesenteric artery, leading to ischemia of an abdominal organ. Which of the following organs is most likely affected?
Scarpa's fascia gets attached to which of the following?
What vessel is responsible for the venous drainage of the liver into the inferior vena cava?
A 67-year-old man has severe cirrhosis of the liver. He most likely has enlarged anastomoses between which of the following pairs of veins?
Practice by Chapter
Anterior Abdominal Wall
Practice Questions
Peritoneum and Peritoneal Cavity
Practice Questions
Stomach and Intestines
Practice Questions
Liver, Gallbladder and Biliary Tract
Practice Questions
Pancreas and Spleen
Practice Questions
Kidneys and Suprarenal Glands
Practice Questions
Abdominal Vasculature
Practice Questions
Posterior Abdominal Wall
Practice Questions
Innervation of Abdominal Viscera
Practice Questions
Applied Anatomy and Clinical Correlations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app