Q11
Which of the following insecticides is a natural contact poison?
Q12
Which of the following is covered under spiritual dimension of health?
Q13
The ratio between incidences among exposed and non-exposed persons is called
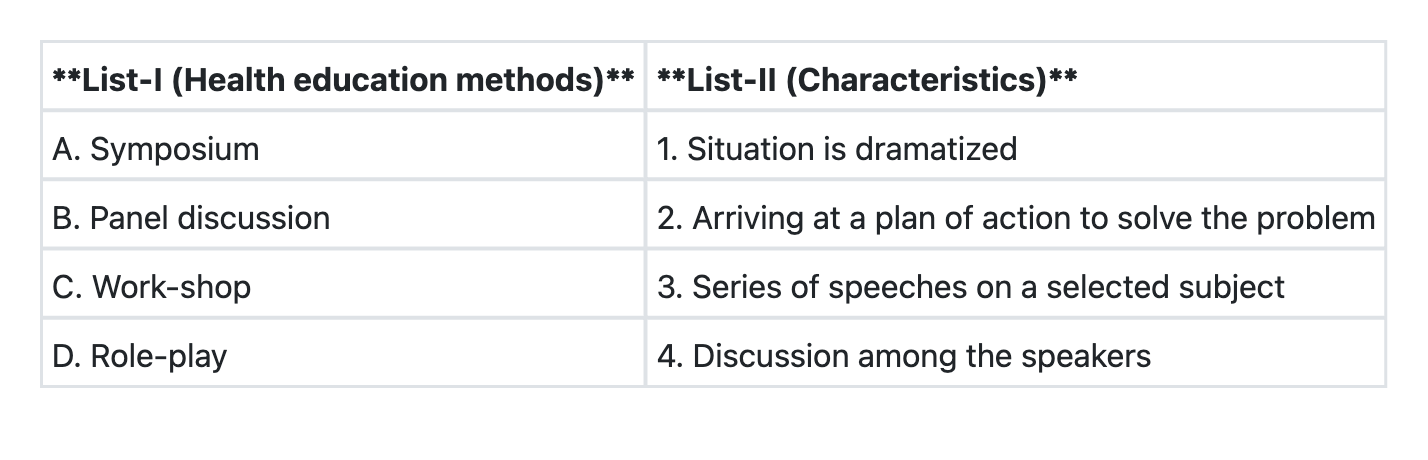
Q14
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q15
A new drug is to be evaluated for its therapeutic effect. The best study design will be.
Q16
Consider the following criteria for a "screening test" : 1. Disease should have a latent period 2. Condition (disease) should be rare 3. Disease should be amenable to treatment Which of the above must be satisfied before including a screening test into any programme?
Q17
"Risk ratio" is also known as:
Q18
Consider the following characteristics of biological agents : 1. Infectivity 2. Pathogenicity 3. Virulence 4. Communicability Among the above characteristics, which are used to measure the ability of biological agents to induce clinically apparent illness?
Q19
"Mid-year population" is not the denominator of which mortality rate?
Q20
The best indicator for the measurement of "completed family size"; that is the number of children a woman would have through her reproductive years is