All (202)Anatomy (16)Anesthesiology (2)Biochemistry (12)Community Medicine (16)Dermatology (5)ENT (5)Forensic Medicine (10)Internal Medicine (25)Microbiology (13)Obstetrics and Gynecology (5)Ophthalmology (9)Orthopaedics (4)Pathology (10)Pediatrics (12)Pharmacology (16)Physiology (12)Psychiatry (6)Radiology (7)Surgery (17)
Q151
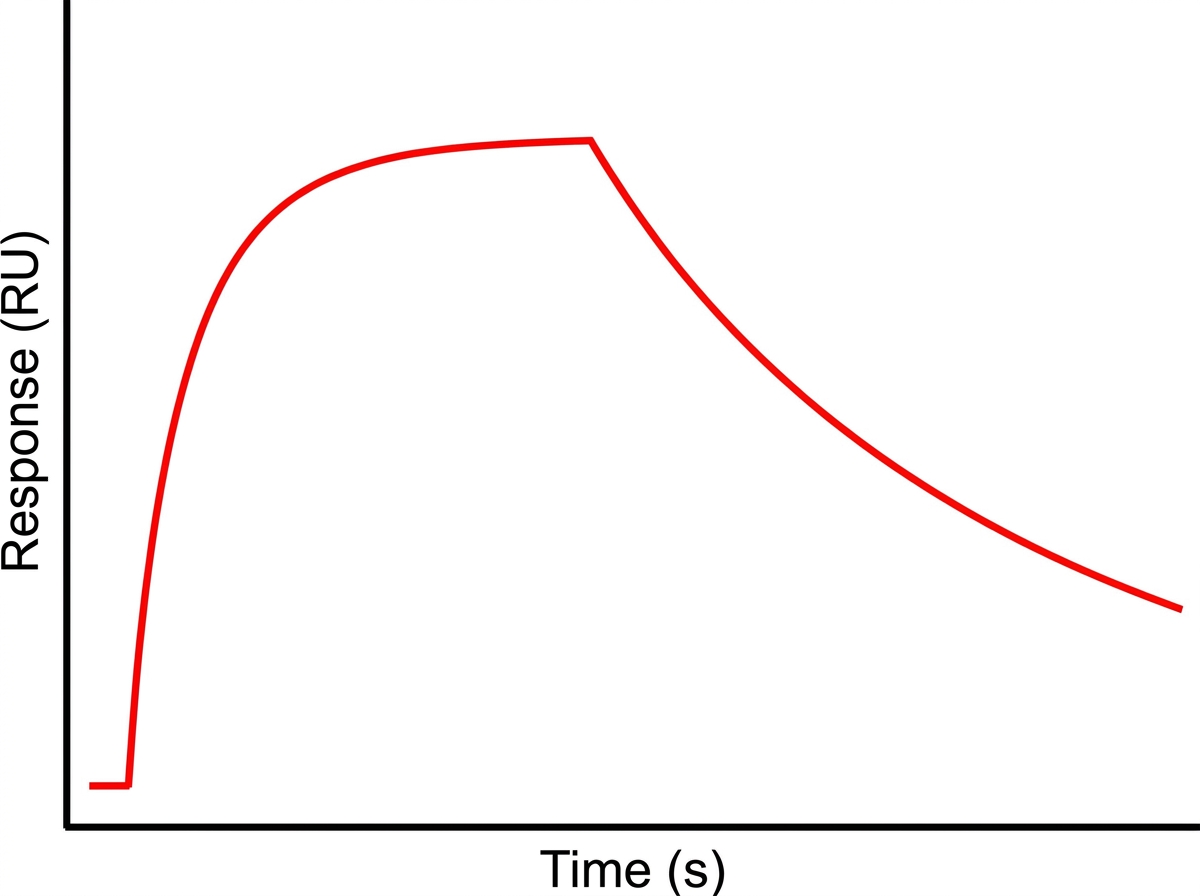
What is the technique shown in the graph that demonstrates antibody-antigen interaction and response kinetics?