INI-CET 2021 — Surgery
7 Previous Year Questions with Answers & Explanations
Which among the following is not used in post laryngectomy rehabilitation?
Which of the following findings appear late in compartment syndrome?
A 12-year-old presented with fever and difficulty swallowing. He had swelling in the marked region and was advised to undergo tonsillectomy. Post-surgery the gauze continued to soak with blood. Which of the following vessels must have been injured?
A 55-year-old female patient presented with a $4 \times 3 \mathrm{~cm}$ lump in the right upper outer quadrant, with no axillary lymph node involvement. Mammography revealed BIRADS 4b staging. She underwent breast conservation surgery, and the final HPE report showed high nuclear-grade DCIS with necrosis and 10 mm margin clearance. What is the further management?
You are suturing a laceration in the ER using the interrupted suturing technique. What is the angle of needle placement?
A 26 year old male patient was brought to the emergency department with abdominal pain and obstipation for 3 days. He gives a history of bull gore to the abdomen 3 days back. His chest X-ray is given below. What is the probable diagnosis?
A 50 year old male patient came to the outpatient department with complaints of hematuria. A 2 x 2 cm bladder mass is seen which is low grade transitional cell carcinoma. Which among the following is the ideal management?
INI-CET 2021 - Surgery INI-CET Practice Questions and MCQs
Question 1: Which among the following is not used in post laryngectomy rehabilitation?
- A. Tracheostomy tube (Correct Answer)
- B. Esophageal speech
- C. Tracheoesophageal puncture
- D. Electrolarynx
Explanation: ***Tracheostomy tube*** - Following total laryngectomy, the **trachea is permanently diverted** to form a permanent stoma in the neck for breathing. - In the context of **post-laryngectomy rehabilitation**, the focus is on **voice restoration** methods rather than airway management devices. - While laryngectomy tubes or stoma buttons may be used temporarily for **stoma care** (preventing stenosis, maintaining patency), traditional **tracheostomy tubes are not part of voice rehabilitation** protocols. - The patient breathes directly through the permanent stoma, and rehabilitation centers on restoring communication ability. *Esophageal speech* - **Esophageal speech** is a voice rehabilitation method where air is injected into the esophagus and then expelled, vibrating the pharyngoesophageal segment to produce sound. - It requires no external devices, only extensive training, and can provide functional voice for communication. - This is one of the **three main voice restoration options** after laryngectomy. *Tracheoesophageal puncture* - **Tracheoesophageal puncture (TEP)** with voice prosthesis is the **gold standard** for voice rehabilitation post-laryngectomy. - A small fistula is created between trachea and esophagus, and a one-way valve (voice prosthesis) is inserted. - Air from the lungs is diverted through the prosthesis into the esophagus, vibrating the pharyngoesophageal segment to produce speech. - Provides the **most natural-sounding voice** among rehabilitation options. *Electrolarynx* - An **electrolarynx** is an external, battery-operated device held against the neck or placed intraorally that generates vibrations. - The vibrations are articulated by the mouth and tongue to produce speech. - Provides **immediate communication** post-laryngectomy, though the voice quality is mechanical or robotic.
Question 2: Which of the following findings appear late in compartment syndrome?
- A. Paralysis
- B. Pain on passive stretch
- C. Pulselessness (Correct Answer)
- D. Pallor
Explanation: ***Pulselessness*** - **Pulselessness** is a very late and ominous sign in compartment syndrome, indicating severe arterial compromise that has progressed beyond simple venous and lymphatic outflow obstruction. - Its presence suggests **irreversible tissue damage** has likely already occurred due to prolonged ischemia. *Paralysis* - **Paralysis** is a late sign, indicating significant nerve ischemia and damage due to sustained pressure within the compartment. - While it's a serious finding, it typically appears before pulselessness, as nerves are sensitive to ischemia but arteries are more resistant to complete occlusion until very high pressures are reached. *Pain on passive stretch* - **Pain on passive stretch** is considered one of the earliest and most reliable clinical signs of early compartment syndrome. - It results from the stretching of ischemic muscle fibers within the confined compartment. *Pallor* - **Pallor** (skin paleness) is also a relatively late sign, occurring when capillary perfusion is significantly reduced due to rising intracompartmental pressure. - It usually manifests when the pressure is high enough to restrict blood flow but often precedes the complete absence of pulses.
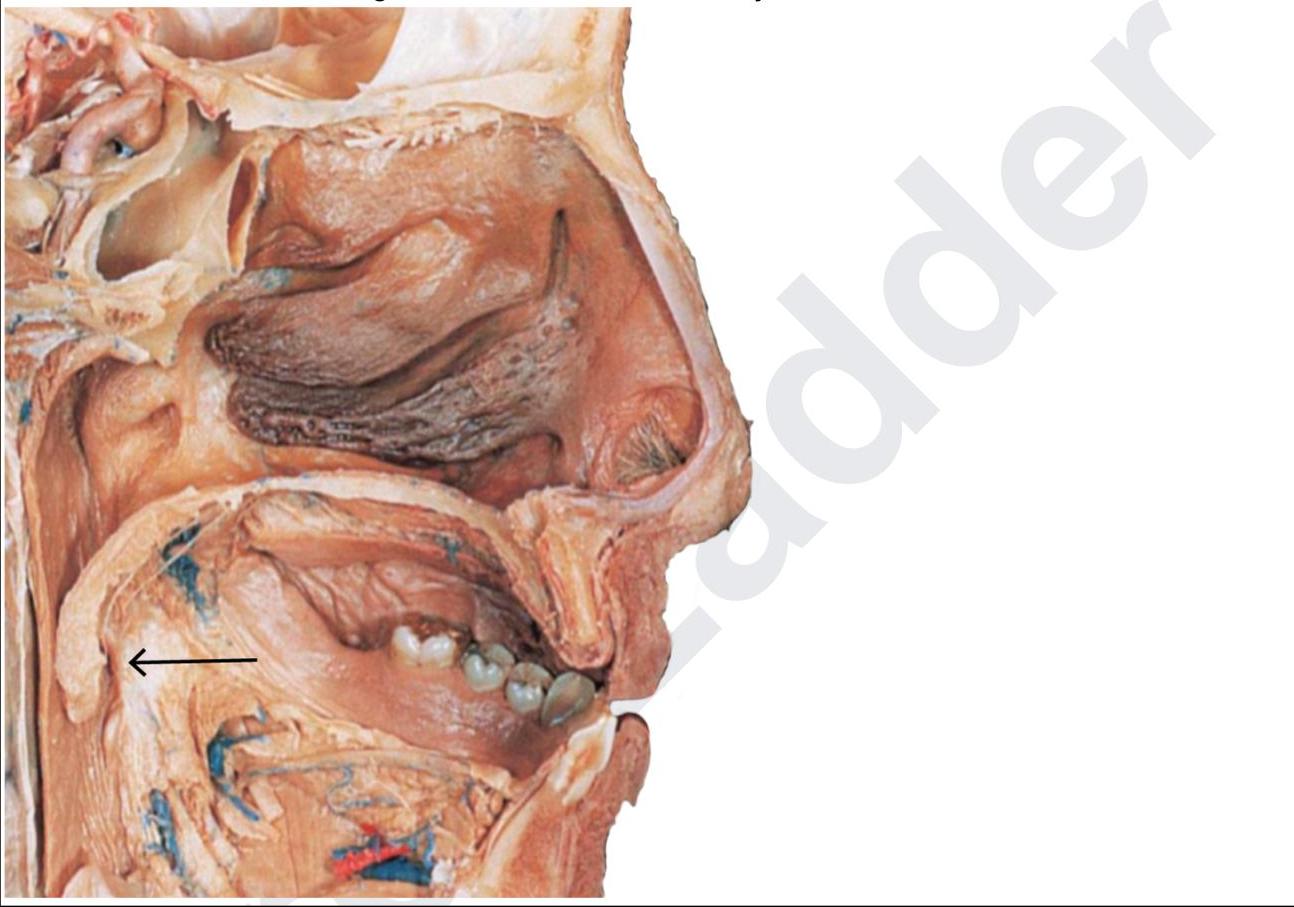
Question 3: A 12-year-old presented with fever and difficulty swallowing. He had swelling in the marked region and was advised to undergo tonsillectomy. Post-surgery the gauze continued to soak with blood. Which of the following vessels must have been injured?
- A. Ascending pharyngeal artery
- B. Tonsillar branch of facial artery
- C. Retromandibular vein
- D. Paratonsillar vein (Correct Answer)
Explanation: ***Paratonsillar vein*** - The **paratonsillar vein**, also known as the **external palatine vein**, is the major vein draining the palatine tonsil and usually the primary source of **post-tonsillectomy hemorrhage**. - Its superficial location and tendency to be large and thin-walled make it particularly vulnerable to injury during **tonsillectomy**, leading to persistent bleeding. *Ascending pharyngeal artery* - The ascending pharyngeal artery contributes to the blood supply of the tonsil, but it is a **deep-seated artery** that is less frequently injured during tonsillectomy compared to the paratonsillar vein. - While its injury could lead to significant bleeding, it's not the most common vascular source of hemorrhage in this context. *Tonsillar branch of facial artery* - The **tonsillar branch of the facial artery** is a significant arterial supply to the tonsil. However, arterial bleeding is typically more pulsatile and rapid, whereas persistent soaking of gauze suggests venous bleeding. - While injury to this artery can occur, the **paratonsillar vein** is a more common source of persistent oozing hemorrhage post-tonsillectomy. *Retromandibular vein* - The **retromandibular vein** is located posterior to the mandible and is not directly associated with the tonsillar bed. - Injury to this vein during a **tonsillectomy** is highly unlikely due to its anatomical position.
Question 4: A 55-year-old female patient presented with a $4 \times 3 \mathrm{~cm}$ lump in the right upper outer quadrant, with no axillary lymph node involvement. Mammography revealed BIRADS 4b staging. She underwent breast conservation surgery, and the final HPE report showed high nuclear-grade DCIS with necrosis and 10 mm margin clearance. What is the further management?
- A. Follow up 6 monthly for 2 years and then yearly follow up
- B. Trastuzumab therapy
- C. Adjuvant chemotherapy
- D. Adjuvant radiotherapy (Correct Answer)
Explanation: ***Adjuvant radiotherapy*** - For **high-grade DCIS** with necrosis after breast conservation surgery, adjuvant radiotherapy significantly reduces the risk of **local recurrence** (by approximately 50%). - Even with adequate margin clearance (10 mm), radiotherapy is recommended to treat **potential residual microscopic disease** elsewhere in the breast tissue. - This is the **standard of care** for high-grade DCIS post-BCS, particularly when necrosis is present. *Follow up 6 monthly for 2 years and then yearly follow up* - While regular follow-up is essential for all breast cancer patients, it is **not sufficient alone** for high-grade DCIS treated with breast conservation. - **Adjuvant radiotherapy** is necessary to reduce recurrence risk before initiating the follow-up schedule. *Trastuzumab therapy* - **Trastuzumab** is specifically indicated for **HER2-positive invasive breast cancer**. - The patient has **DCIS**, which is **non-invasive (in situ)**, making trastuzumab inappropriate. - There is no role for targeted therapy in DCIS management. *Adjuvant chemotherapy* - **Adjuvant chemotherapy** is generally reserved for **invasive breast cancers**, especially those with high-risk features like lymph node involvement or aggressive tumor biology. - For **DCIS**, even high-grade with necrosis, chemotherapy is **not indicated** as it provides no proven benefit for non-invasive disease.
Question 5: You are suturing a laceration in the ER using the interrupted suturing technique. What is the angle of needle placement?
- A. 80 degrees
- B. 70 degrees
- C. 60 degrees
- D. 90 degrees (Correct Answer)
Explanation: ***90 degrees*** - Placing the needle at a **90-degree angle** to the skin surface ensures that the suture comes out perpendicular to the skin edge, creating an **eversion of the wound edges**. - This perpendicular entry allows for an equal amount of tissue to be grasped on both sides of the wound, promoting proper **wound approximation** and healing. *80 degrees* - An 80-degree angle, while close, would not provide the ideal **perpendicular entry** needed to properly evert the wound edges. - This slight deviation from 90 degrees could lead to less precise **tissue approximation** and potentially an inverted wound edge. *70 degrees* - A 70-degree angle is too shallow and would result in the suture entering the wound more tangentially, leading to **inverted wound edges**. - **Inverted wound edges** hinder optimal healing and can result in a less aesthetically pleasing scar. *60 degrees* - A 60-degree angle is significantly too shallow, which would cause the suture to be placed too superficially and horizontally, resulting in **poor wound edge eversion**. - This angle would make it difficult to adequately appose the deeper dermal layers, compromising **tensile strength** and increasing the risk of scar formation.
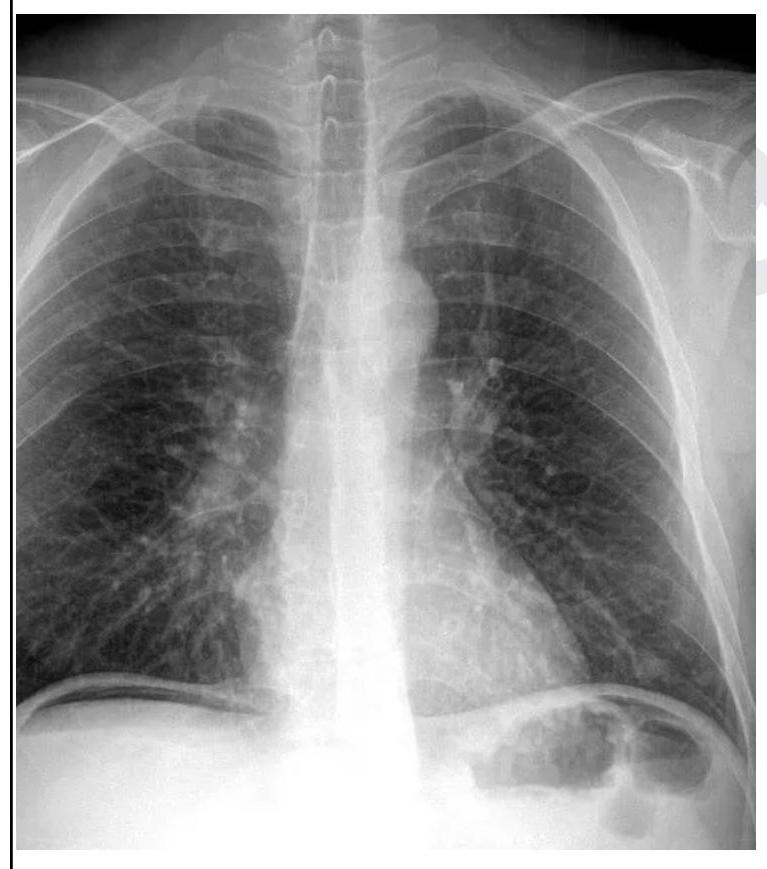
Question 6: A 26 year old male patient was brought to the emergency department with abdominal pain and obstipation for 3 days. He gives a history of bull gore to the abdomen 3 days back. His chest X-ray is given below. What is the probable diagnosis?
- A. Hemothorax
- B. Hollow viscus perforation (Correct Answer)
- C. Pneumothorax
- D. Intestinal obstruction
Explanation: ***Hollow viscus perforation*** - The chest X-ray clearly shows **free air under the diaphragm** (pneumoperitoneum), which is a hallmark sign of a perforated hollow viscus in the abdomen. - The history of **bull gore to the abdomen** and subsequent abdominal pain and obstipation further supports a traumatic perforation of a stomach or intestinal segment. *Hemothorax* - Hemothorax would present as **fluid in the pleural space**, typically seen as blunting of the costophrenic angles or an effusion on X-ray, which is not evident here. - While trauma can cause hemothorax, the prominent finding on this X-ray is intra-abdominal air, not intrathoracic fluid. *Pneumothorax* - Pneumothorax is characterized by the presence of **air in the pleural space**, leading to lung collapse and absence of lung markings in the affected area, which is not observed on this X-ray. - The air seen is clearly **below the diaphragm**, indicating intra-abdominal free air, not air in the chest cavity surrounding the lung. *Intestinal obstruction* - Intestinal obstruction typically presents with **dilated bowel loops** and **air-fluid levels** on an abdominal X-ray, along with abdominal pain and obstipation. - While the patient has obstipation, the primary X-ray finding is free air under the diaphragm, which is not characteristic of an uncomplicated intestinal obstruction.
Question 7: A 50 year old male patient came to the outpatient department with complaints of hematuria. A 2 x 2 cm bladder mass is seen which is low grade transitional cell carcinoma. Which among the following is the ideal management?
- A. Resection with ileal conduit
- B. Partial cystectomy with bladder reconstruction
- C. Neoadjuvant chemotherapy
- D. Transurethral resection of the tumour (Correct Answer)
Explanation: ***Transurethral resection of the tumour*** - For a **low-grade transitional cell carcinoma** that is 2x2 cm and thus considered small and localized, **transurethral resection of the tumor (TURBT)** is the initial and often definitive treatment. - This procedure allows for both **diagnosis** by obtaining tissue samples and **complete removal** of the visible tumor. *Resection with ileal conduit* - This option, involving a **radical cystectomy** and urinary diversion, is a more aggressive treatment reserved for **invasive, high-grade, or recurrent bladder cancers** that cannot be managed by less invasive means. - It would be **overtreatment** for a low-grade, relatively small bladder mass. *Partial cystectomy with bladder reconstruction* - **Partial cystectomy** is considered for solitary, muscle-invasive tumors located away from critical areas (like the trigone) when bladder preservation is desirable. - It is generally not the first-line treatment for **non-muscle-invasive, low-grade tumors** due to the potential for recurrence in the remaining bladder and the morbidity of open surgery compared to TURBT. *Neoadjuvant chemotherapy* - **Neoadjuvant chemotherapy** is typically administered before radical cystectomy for **muscle-invasive bladder cancer** to improve oncologic outcomes. - It is not indicated for **low-grade, non-muscle-invasive bladder cancer** which is usually managed surgically first, without systemic chemotherapy.