INI-CET 2021 — Physiology
11 Previous Year Questions with Answers & Explanations
The relaxation of the intestinal segment distal to the segment with the bolus of food during peristalsis is because of?
Milk production in pregnancy is inhibited by :
All of the following increases gastric acid secretion except?
Pacinian corpuscle is stimulated by which of the following?
An individual is in an environment of a temperature of 47°C. What is the mechanism of heat loss?
Which among the following has the highest airway resistance?
If the contractility of the heart is decreased, which of the following is seen ?
All of the following substances have decreased concentration on the luminal side of the proximal convoluted tubule except:
A woman with right-sided loss of sensations of both the upper and lower limb complains of shooting pain from her fingers to the right shoulder and a burning sensation when touching cold water. Motor functions are normal. Which of the following structures is likely to be involved?
Identify the pathology from the given flow-volume loop:
INI-CET 2021 - Physiology INI-CET Practice Questions and MCQs
Question 1: The relaxation of the intestinal segment distal to the segment with the bolus of food during peristalsis is because of?
- A. Substance P
- B. Norepinephrine from adrenergic fibers
- C. VIP
- D. Nitric oxide (NO) (Correct Answer)
Explanation: ***Nitric oxide (NO)*** - **Nitric oxide (NO)** is a key **inhibitory neurotransmitter** that causes relaxation of the smooth muscle distal to the bolus during peristalsis, allowing the food to move forward. - Along with **Vasoactive Intestinal Peptide (VIP)**, NO mediates the **descending relaxation reflex** in the gut, which is essential for effective propulsion. *Substance P* - **Substance P** is an **excitatory neurotransmitter** that primarily mediates contraction of the smooth muscle proximal to the bolus during peristalsis. - It works synergistically with **acetylcholine** to initiate the muscular squeeze that propels food. *Norepinephrine from adrenergic fibers* - **Norepinephrine** is the primary neurotransmitter released by **sympathetic adrenergic fibers** in the gastrointestinal tract. - While sympathetic stimulation generally **inhibits gastrointestinal motility**, this is a systemic effect that reduces overall gut activity rather than causing the specific segmental relaxation distal to a bolus during peristalsis. - The descending relaxation during peristalsis is mediated by **intrinsic enteric neurons** (releasing NO and VIP), not by extrinsic sympathetic innervation. *VIP* - **Vasoactive Intestinal Peptide (VIP)** is an **inhibitory neurotransmitter** that causes relaxation of smooth muscle in the gut. - While VIP does contribute to descending relaxation, **nitric oxide (NO)** is considered a more significant and primary mediator of this specific relaxation during peristalsis.
Question 2: Milk production in pregnancy is inhibited by :
- A. Low luteinizing hormone
- B. Low thyroid-stimulating hormone
- C. High estrogen (Correct Answer)
- D. Human somatomammotropin
Explanation: ***High estrogen*** - High levels of **estrogen** and progesterone during pregnancy inhibit milk production by blocking the action of **prolactin** on the mammary glands. - After delivery, the sudden drop in these hormones removes the inhibition, allowing prolactin to stimulate **lactogenesis**. *Low luteinizing hormone* - **Luteinizing hormone (LH)** is primarily involved in ovulation and corpus luteum formation, not directly in the inhibition of milk production. - Low LH levels would impact fertility but not have a direct inhibitory effect on lactation. *Low thyroid-stimulating hormone* - **Thyroid-stimulating hormone (TSH)** regulates thyroid function, which can indirectly affect metabolism and overall well-being. - While **hypothyroidism** can impact milk supply, low TSH itself is not a direct inhibitor of milk production. *Human somatomammotropin* - **Human placental lactogen (HPL)**, also known as human chorion somatomammotropin, is produced by the placenta. - It promotes mammary gland development and has weak lactogenic properties but does not inhibit milk production.
Question 3: All of the following increases gastric acid secretion except?
- A. Acetylcholine
- B. Histamine
- C. Serotonin (Correct Answer)
- D. Gastrin
Explanation: ***Serotonin*** - **Serotonin** (5-HT) is primarily known for its roles in gastrointestinal motility and CNS function, but it does not directly stimulate **gastric acid secretion**. - While it can influence gastric function indirectly, it is not a direct secretagogue for **parietal cells**. *Acetylcholine* - **Acetylcholine** (ACh), released from parasympathetic nerve endings, directly stimulates **parietal cells** to secrete hydrochloric acid. - It also enhances the release of **histamine** and **gastrin**, both of which promote acid secretion. *Histamine* - **Histamine**, released from enterochromaffin-like (ECL) cells in the gastric mucosa, is a potent stimulator of **gastric acid secretion**. - It acts on **H2 receptors** on parietal cells, leading to increased acid production. *Gastrin* - **Gastrin**, a hormone produced by G cells in the pyloric antrum, is a powerful stimulator of **gastric acid secretion**. - It acts directly on **parietal cells** and also promotes **histamine release** from ECL cells.
Question 4: Pacinian corpuscle is stimulated by which of the following?
- A. Pain
- B. Temperature
- C. Touch
- D. Pressure (Correct Answer)
Explanation: ***Pressure*** - **Pacinian corpuscles** are rapidly adapting mechanoreceptors that detect **deep pressure** and **vibrations**. - Their layered, onion-like structure allows them to be very sensitive to rapid changes in pressure. *Pain* - **Pain** is primarily detected by **nociceptors**, which are free nerve endings, not Pacinian corpuscles. - Nociceptors respond to various noxious stimuli, including mechanical, thermal, and chemical. *Temperature* - **Temperature** changes are detected by **thermoreceptors**, such as Krause end bulbs for cold and Ruffini endings for warmth, not Pacinian corpuscles. - These receptors have specific temperature ranges over which they are active. *Touch* - **Touch** sensation is broadly detected by several mechanoreceptors, including **Meissner's corpuscles** (light touch), **Merkel discs** (sustained touch), and hair follicle receptors. - While Pacinian corpuscles contribute to sensing touch through deep pressure, they are not the primary receptors for general light or sustained touch.
Question 5: An individual is in an environment of a temperature of 47°C. What is the mechanism of heat loss?
- A. Conduction
- B. Radiation
- C. Sweating (Correct Answer)
- D. Convection
Explanation: ***Sweating*** - In an environment where the ambient temperature (47°C) is **higher than body temperature**, heat can only be lost through the evaporation of sweat. - **Evaporation** is the primary mechanism for cooling the body in hot environments when other forms of heat loss become ineffective or even cause heat gain. *Conduction* - **Conduction** involves the transfer of heat through direct contact between surfaces. - In an environment hotter than the body, conduction would cause **heat gain** by the body, not heat loss. *Radiation* - **Radiation** involves the transfer of heat in the form of electromagnetic waves. - When the ambient temperature is higher than body temperature, the body will **absorb radiant heat** from the environment, leading to heat gain, not loss. *Convection* - **Convection** is the transfer of heat through the movement of fluids (air or water). - In an environment with a temperature of 47°C, convection would cause **heat gain** as the surrounding hot air transfers heat to the body.
Question 6: Which among the following has the highest airway resistance?
- A. Alveolar duct
- B. Respiratory bronchioles
- C. Bronchi (Correct Answer)
- D. Small bronchioles
Explanation: ***Bronchi (Medium-sized bronchi)*** - The **medium-sized bronchi** (approximately 4th-8th generation airways) contribute the **highest proportion to total airway resistance** in the tracheobronchial tree. - At this level, airways are still relatively **narrow** but arranged more in **series** rather than parallel, concentrating resistance. - This is the point of **maximum resistance** before the extensive branching of smaller airways creates parallel pathways. - Accounts for approximately **40-50% of total airway resistance** during normal breathing. *Small bronchioles* - While individual small bronchioles (<1 mm diameter) have narrow lumens, they branch extensively into **thousands of parallel airways**. - This creates an **enormous total cross-sectional area** (up to 20x larger than trachea), which dramatically **reduces total resistance**. - According to principles of parallel resistance, total resistance decreases as more parallel pathways are added: 1/R_total = 1/R₁ + 1/R₂ + ... + 1/Rₙ - Despite small individual diameter, collective parallel arrangement makes them **low resistance** pathways. *Alveolar ducts* - Have the **largest cumulative cross-sectional area** in the entire respiratory system. - Airflow velocity is minimal and flow is entirely **laminar**, offering negligible resistance. - These are part of the respiratory zone where gas exchange occurs primarily by diffusion. *Respiratory bronchioles* - Part of the **transitional/respiratory zone** with extensive branching and large total cross-sectional area. - Offer very low resistance due to their **parallel arrangement** and slow airflow velocity. - Contribute minimally to total airway resistance.
Question 7: If the contractility of the heart is decreased, which of the following is seen ?
- A. Increased ejection fraction
- B. Increased stroke work
- C. Decreased stroke volume (Correct Answer)
- D. Increased cardiac output
Explanation: ***Decreased stroke volume*** - A decrease in the **contractility** of the heart directly reduces the force of myocardial contraction. - This weaker contraction results in less blood being ejected from the ventricle per beat, leading to a **decreased stroke volume**. *Increased ejection fraction* - **Ejection fraction** is the percentage of blood ejected from the ventricle with each beat, calculated as (stroke volume / end-diastolic volume) x 100. - When contractility decreases, **stroke volume** decreases, which would typically lead to a *decreased* ejection fraction, not an increased one. *Increased stroke work* - **Stroke work** is a measure of the work done by the ventricle to eject blood, and it depends on both stroke volume and aortic pressure. - With decreased contractility, **stroke volume** falls, which would *decrease* the stroke work, assuming afterload remains constant. *Increased cardiac output* - **Cardiac output** is the product of stroke volume and heart rate (CO = SV x HR). - Since decreased contractility leads to a **decreased stroke volume**, without a compensatory increase in heart rate, cardiac output would *decrease*, not increase.
Question 8: All of the following substances have decreased concentration on the luminal side of the proximal convoluted tubule except:
- A. Glucose
- B. Amino acids
- C. Bicarbonate
- D. Chloride (Correct Answer)
Explanation: ***Chloride*** - As **water and other solutes** are reabsorbed from the proximal tubule, the concentration of **chloride** actually increases in the remaining luminal fluid due to continued water reabsorption. - This increased luminal **chloride concentration** then drives passive reabsorption of chloride later in the tubule. *Glucose* - **Glucose** is almost completely reabsorbed from the tubular lumen by **secondary active transport** in the early part of the proximal tubule. - Therefore, its concentration in the remaining luminal fluid rapidly decreases. *Amino acids* - Similar to glucose, **amino acids** are extensively reabsorbed by **secondary active transport** mechanisms in the proximal tubule. - Consequently, their luminal concentration significantly decreases. *Bicarbonate* - Most **bicarbonate** is reabsorbed in the proximal tubule through a process involving **carbonic anhydrase**, converting it to CO2 and water, which then diffuse into the cell. - This efficient reabsorption results in a substantial decrease in luminal bicarbonate concentration.
Question 9: A woman with right-sided loss of sensations of both the upper and lower limb complains of shooting pain from her fingers to the right shoulder and a burning sensation when touching cold water. Motor functions are normal. Which of the following structures is likely to be involved?
- A. Anterior spinothalamic tract
- B. Spinocerebellar tract
- C. Lateral spinothalamic tract (Correct Answer)
- D. Posterior column
Explanation: ***Lateral spinothalamic tract*** - The symptoms described, such as **loss of sensations**, **shooting pain** (neuropathic pain), and **burning sensation** with cold water (dysesthesia/allodynia), are characteristic of damage to the **spinothalamic tract**, which carries **pain and temperature** sensations. - Involvement of the **right-sided upper and lower limb** indicates a lesion affecting sensory pathways on the ipsilateral side of the body before decussation, or more commonly a contralateral lesion above the level of decussation for the specific tract. Given the symptoms affecting pain and temperature, the lateral spinothalamic tract is the primary candidate. *Anterior spinothalamic tract* - This tract primarily transmits **crude touch** and **pressure** sensations. - While loss of sensation is present, the prominent **shooting pain** and **burning sensation with cold water** are not typically associated with isolated anterior spinothalamic tract lesions. *Spinocerebellar tract* - This tract is responsible for transmitting **proprioceptive information** to the cerebellum for motor coordination. - Damage to the spinocerebellar tracts would manifest as **ataxia** and **incoordination**, not pain or loss of touch/temperature sensation, and motor functions are stated as normal in the patient. *Posterior column* - The posterior column (dorsal column-medial lemniscus pathway) transmits **fine touch**, **vibration**, and **proprioception**. - While a loss of sensation is present, the specific complaints of **shooting pain** and **burning sensation to cold water** are not characteristic of posterior column damage, which would typically present with deficits in discriminative touch, vibratory sense, and position sense.
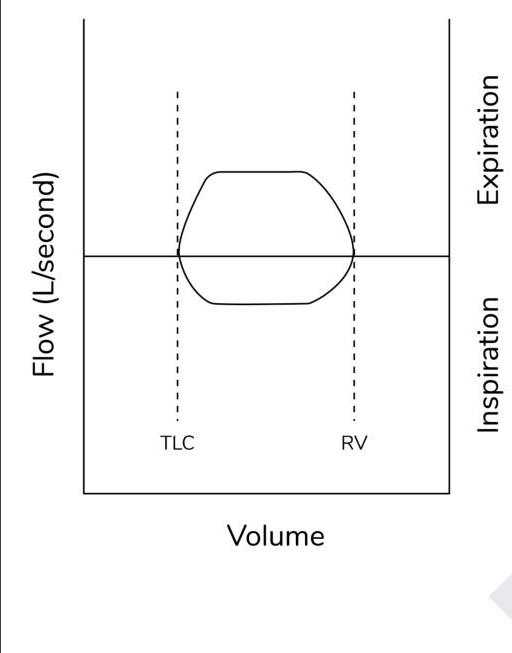
Question 10: Identify the pathology from the given flow-volume loop:
- A. Variable extra thoracic obstruction
- B. Variable intrathoracic obstruction
- C. Fixed distal airway obstruction
- D. Fixed central airway obstruction (Correct Answer)
Explanation: ***Fixed central airway obstruction*** - This flow-volume loop shows **flattening of both the inspiratory and expiratory limbs**, creating a characteristic "box" or "square" shape. - This pattern indicates that airflow is limited equally during both inspiration and expiration, regardless of lung volume changes, which is characteristic of a **fixed central airway obstruction**. - Examples include **tracheal stenosis, tracheal tumors, or fixed goiters** compressing the trachea. *Variable extrathoracic obstruction* - Characterized by flattening of the **inspiratory limb only**, as negative intrathoracic pressure during inspiration exacerbates the obstruction. - The expiratory limb typically remains normal as positive intrathoracic pressure tends to open the airway. - Examples include **vocal cord paralysis or extrathoracic tracheal tumors**. *Variable intrathoracic obstruction* - Characterized by flattening of the **expiratory limb only**, as positive intrathoracic pressure during forced expiration collapses the airway. - The inspiratory limb usually remains normal as negative pressure helps maintain airway patency. - Examples include **intrathoracic tracheal tumors or tracheomalacia**. *Fixed distal airway obstruction* - Fixed obstructions producing the characteristic "box" pattern are typically **central (proximal) lesions in large airways**, not distal. - Distal airway obstructions (like **COPD or asthma**) produce a different flow-volume loop pattern characterized by **decreased peak expiratory flow** and "scooping" or "concave" appearance of the expiratory limb, not the flat bilateral pattern seen here.