All (155)Anatomy (9)Anesthesiology (4)Biochemistry (11)Community Medicine (13)Dermatology (4)ENT (3)Forensic Medicine (7)Internal Medicine (14)Microbiology (7)Obstetrics and Gynecology (15)Ophthalmology (3)Orthopaedics (4)Pathology (14)Pediatrics (7)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (6)
Q61
A female patient having frothy vaginal discharge was found to have a strawberry cervix. Which of the following is the drug of choice?
Q62
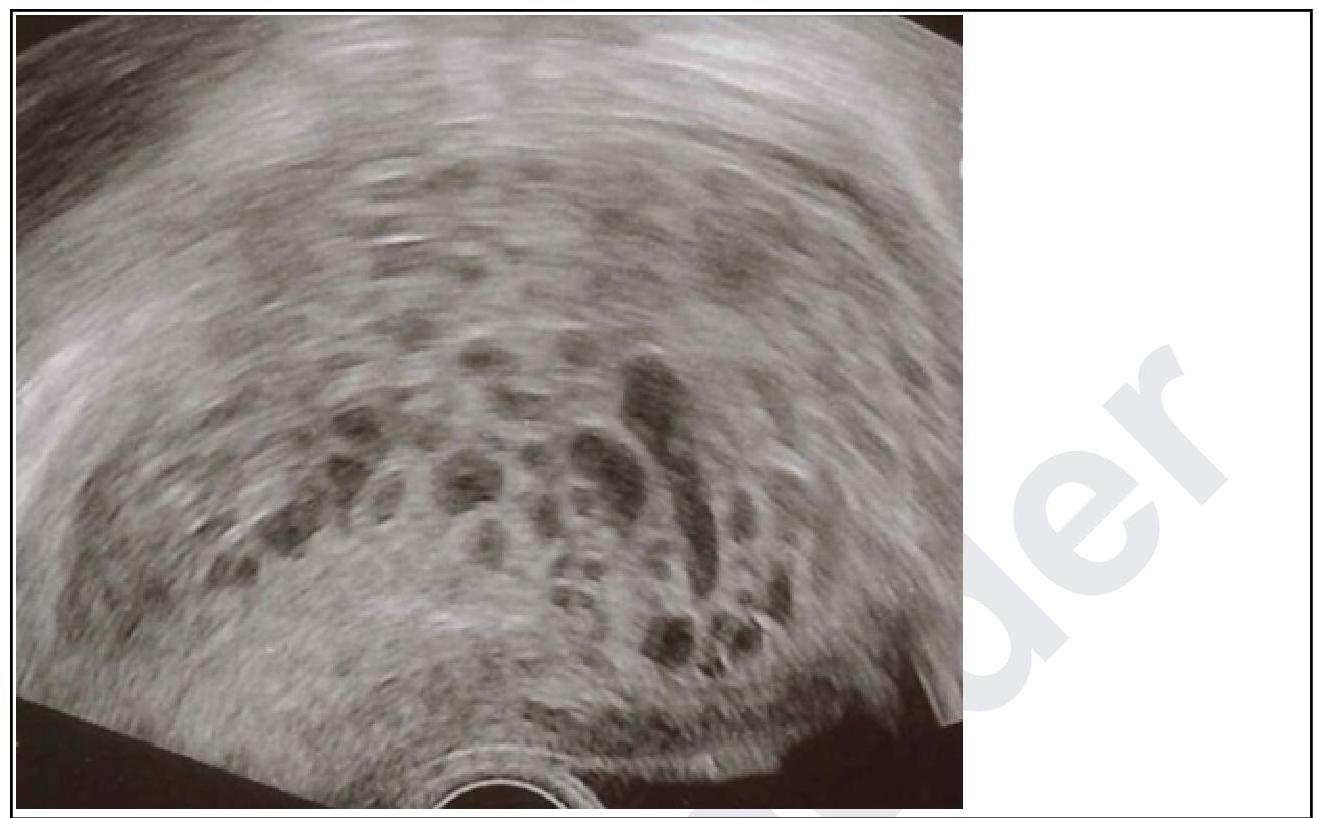
A primigravida in her 10th week of gestation presents with spotting. On examination, the uterus corresponds to 12 weeks. Transvaginal ultrasound was done and it is given below. What is your diagnosis?