All (155)Anatomy (9)Anesthesiology (4)Biochemistry (11)Community Medicine (13)Dermatology (4)ENT (3)Forensic Medicine (7)Internal Medicine (14)Microbiology (7)Obstetrics and Gynecology (15)Ophthalmology (3)Orthopaedics (4)Pathology (14)Pediatrics (7)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (6)
Q131
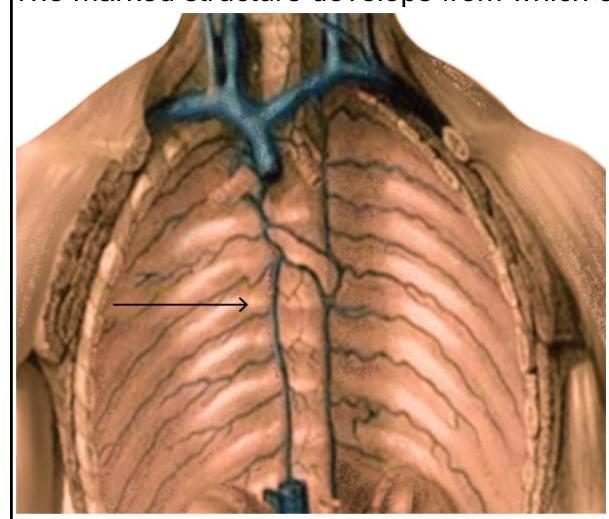
The marked structure develops from which of the following structures?
Q132
Inferior thyroid artery supplies which of the following structures? 1. Thyroid 2. Parathyroid 3. Esophagus 4. Thymus
Q133
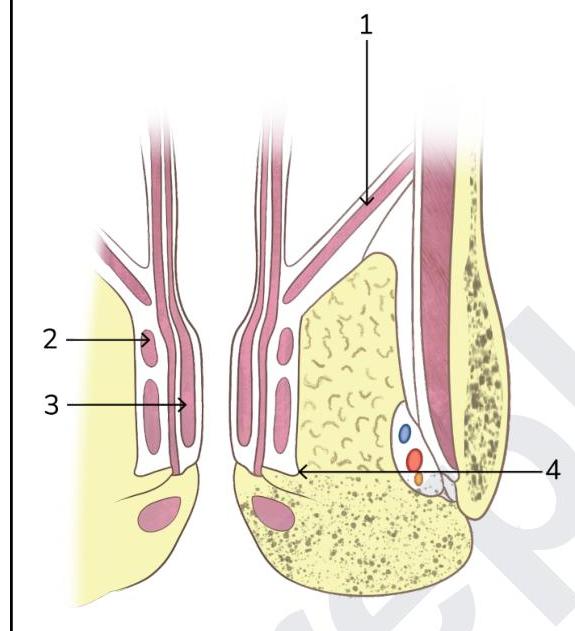
Identify the pelvic diaphragm in the picture given below:
Q134
Third part of vertebral artery is related to which of the following ?
Q135
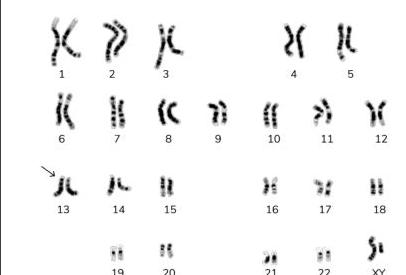
Identify the type of marked chromosome in the given karyotype.