All (155)Anatomy (9)Anesthesiology (4)Biochemistry (11)Community Medicine (13)Dermatology (4)ENT (3)Forensic Medicine (7)Internal Medicine (14)Microbiology (7)Obstetrics and Gynecology (15)Ophthalmology (3)Orthopaedics (4)Pathology (14)Pediatrics (7)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (6)
Q111
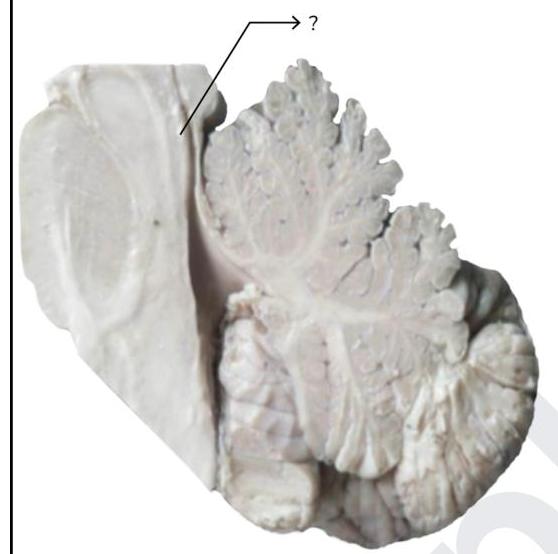
Fibers from the marked structure terminate at which of the following?