All (155)Anatomy (9)Anesthesiology (4)Biochemistry (11)Community Medicine (13)Dermatology (4)ENT (3)Forensic Medicine (7)Internal Medicine (14)Microbiology (7)Obstetrics and Gynecology (15)Ophthalmology (3)Orthopaedics (4)Pathology (14)Pediatrics (7)Pharmacology (14)Physiology (11)Psychiatry (4)Radiology (5)Surgery (6)
Q101
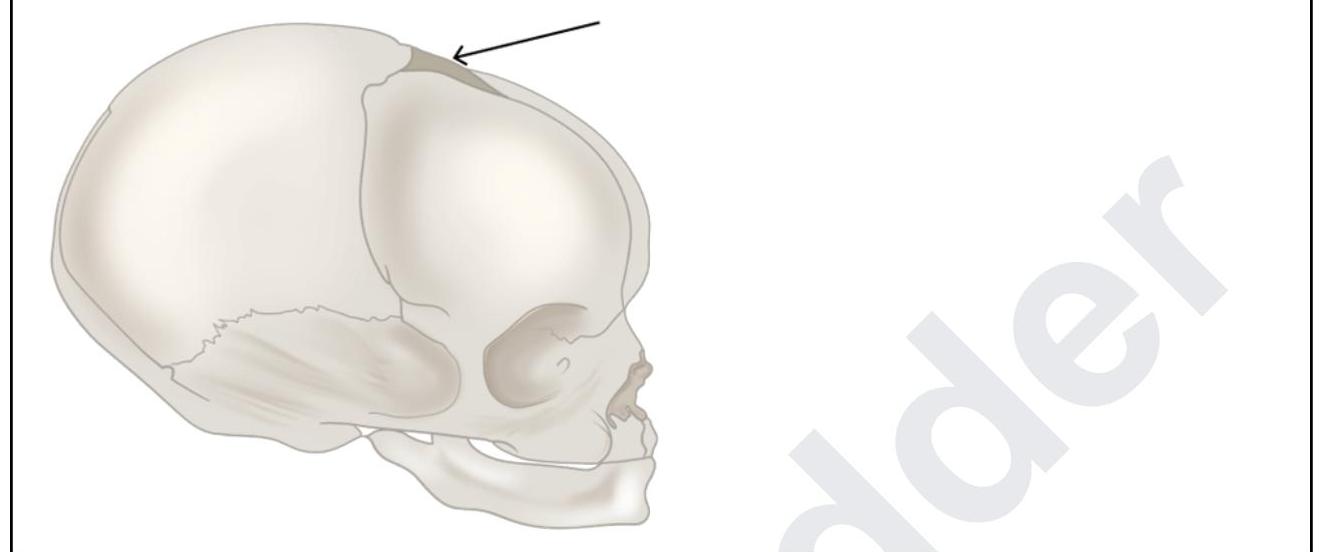
A 6-month-old boy was brought to the casualty with seizures. The pediatrician tries to do CSF sampling. What are the structures punctured by the pediatrician while piercing through the marked structure?