INI-CET 2021 — Obstetrics and Gynecology
16 Previous Year Questions with Answers & Explanations
A pregnant woman at 36 weeks gestation is found to have high blood pressure recording and a urine protein of 3+. Concomitant presence of which of the following symptoms would make you suspect imminent eclampsia? 1. Headache 2. Blurred vision 3. Persistent pedal oedema 4. Epigastric pain
Arrange the following in sequential order with regards to the steps of collection of samples for pap smear testing: Use posterior vaginal wall retractor Take the sample Make smear on a slide Fix the smear
Which of the following is a part of AMTSL?
Which of the following is not a cause of secondary amenorrhea?
What is the minimum percentage for normal sperm morphology according to WHO criteria in seminal fluid analysis?
Which of the following instruments are used in the caesarean section? 1. Bard-Parker blade 2. Doyen's retractor 3. Cusco's speculum 4. Allis forceps 5. Shirodkar's uterine clamp 6. Green Armytage forceps
What is the normal cervical length?
Which of the following symptoms are seen in endometriosis? 1. Infertility 2. Dysmenorrhea 3. Vaginal discharge 4. Vaginal bleeding
A female patient having frothy vaginal discharge was found to have a strawberry cervix. Which of the following is the drug of choice?
A primigravida in her 10th week of gestation presents with spotting. On examination, the uterus corresponds to 12 weeks. Transvaginal ultrasound was done and it is given below. What is your diagnosis?
INI-CET 2021 - Obstetrics and Gynecology INI-CET Practice Questions and MCQs
Question 1: A pregnant woman at 36 weeks gestation is found to have high blood pressure recording and a urine protein of 3+. Concomitant presence of which of the following symptoms would make you suspect imminent eclampsia? 1. Headache 2. Blurred vision 3. Persistent pedal oedema 4. Epigastric pain
- A. 1,2,3,4
- B. 2 and 4 only
- C. 1,2,3
- D. 1 and 2 only (Correct Answer)
Explanation: ***1 and 2 only*** - **Headache** (severe, persistent, frontal or occipital) and **blurred vision** (scotomas, photophobia, or visual field defects) are the classic **neurological symptoms** indicating cerebral irritation and vasospasm that directly precede eclamptic seizures. - These symptoms reflect **imminent CNS involvement** and are the strongest predictors of impending seizure, requiring urgent intervention (magnesium sulfate prophylaxis, delivery planning). - While other symptoms indicate severe pre-eclampsia, these neurological signs specifically herald **imminent eclampsia**. *2 and 4 only* - **Blurred vision** is indeed a key warning sign, and **epigastric pain** (right upper quadrant pain) is an important symptom of severe pre-eclampsia indicating hepatic capsule distension or subcapsular hematoma. - However, this option misses **headache**, which is one of the most critical neurological warning signs of imminent seizure. Epigastric pain indicates hepatic involvement (severe disease) but is not as directly predictive of immediate seizure onset as the combination of headache and visual disturbances. *1,2,3,4* - While headache, blurred vision, and epigastric pain are all features of severe pre-eclampsia, **persistent pedal edema** is extremely common in normal pregnancy and pre-eclampsia (present in >80% of cases) and is **not a specific indicator of imminent eclampsia**. - Generalized edema alone does not indicate imminent seizure risk and is too non-specific to be grouped with the acute neurological warning signs. *1,2,3* - **Headache** and **blurred vision** are the correct neurological indicators of imminent eclampsia. - However, **persistent pedal edema** is very common in pre-eclampsia and not specific for imminent eclamptic seizure risk. It does not have the same predictive value as severe headache or acute visual disturbances for identifying patients at immediate risk of convulsion.
Question 2: Arrange the following in sequential order with regards to the steps of collection of samples for pap smear testing: Use posterior vaginal wall retractor Take the sample Make smear on a slide Fix the smear
- A. 1,2,4,3
- B. 3,1,2,4
- C. 1,2,3,4 (Correct Answer)
- D. 2,1,3,4
Explanation: ***1,2,3,4*** - The correct sequence for collecting a Pap smear involves first **visualizing the cervix** using a posterior vaginal wall retractor, then **taking the sample** (e.g., using a broom or spatula and brush), followed by **making a smear on a slide** and finally **fixing the smear** to preserve the cells. - This sequential order ensures proper cell collection and preservation for accurate cytological examination. *1,2,4,3* - This option incorrectly places **fixing the smear** before **making the smear on the slide**. Cells must first be spread onto the slide before they can be fixed. - Fixing an un-smeared sample or attempting to smear after fixing would lead to an inadequate or damaged specimen. *3,1,2,4* - This sequence incorrectly starts with **making a smear on a slide** before any sample has been collected or the cervix visualized. - One cannot make a smear without first taking a sample and accessing the cervix via a retractor. *2,1,3,4* - This option incorrectly states that **taking the sample** occurs before **using a posterior vaginal wall retractor**. The retractor is essential for proper visualization and access to the cervix to obtain a quality sample. - Attempting to take a sample without proper visualization would lead to an inadequate or incorrect specimen collection.
Question 3: Which of the following is a part of AMTSL?
- A. Uterine massage
- B. Controlled cord traction (Correct Answer)
- C. Early cord clamping
- D. Uterotonics after delivery of placenta
Explanation: ***Controlled cord traction*** - **Controlled cord traction (CCT)** is a key component of Active Management of Third Stage of Labor (AMTSL) performed during placental delivery. - This technique involves applying gentle, sustained traction to the umbilical cord while simultaneously providing counter-traction to the fundus (Brandt-Andrews maneuver) to prevent **uterine inversion**. - CCT is performed after administering a uterotonic and is the primary active maneuver for delivering the placenta. *Uterine massage* - **Uterine massage** is also a component of AMTSL, but it is performed **after placental delivery** to ensure adequate uterine contraction and prevent postpartum hemorrhage. - The three components of AMTSL per WHO recommendations are: (1) Uterotonic administration, (2) Controlled cord traction, (3) Uterine massage after placental delivery. - While technically part of AMTSL, **controlled cord traction** is the more specific answer as it refers to the active maneuver during placental separation and delivery itself. *Early cord clamping* - **Early cord clamping** (within 60 seconds of birth) has been removed from AMTSL recommendations in favor of **delayed cord clamping** (1-3 minutes or when pulsation stops). - Current WHO guidelines recommend delayed cord clamping for all births while still performing AMTSL, as delayed clamping provides neonatal benefits without increasing maternal hemorrhage risk. *Uterotonics after delivery of placenta* - **Uterotonics** (oxytocin 10 IU IM/IV) are administered **within 1 minute of birth** of the baby, which is *before* placental delivery, not after. - This prophylactic administration is the cornerstone of AMTSL and reduces postpartum hemorrhage risk by approximately 60%. - Administering uterotonics *after* placental delivery does not constitute proper AMTSL timing.
Question 4: Which of the following is not a cause of secondary amenorrhea?
- A. Kallman syndrome (Correct Answer)
- B. Asherman's syndrome
- C. Sheehan's syndrome
- D. Turner's mosaic
Explanation: ***Kallman syndrome*** - This is a cause of **primary amenorrhea** because it involves congenital **GnRH deficiency**, preventing the onset of puberty and menstruation from the beginning. - Patients typically present with failure of pubertal development and **anosmia** (inability to smell). *Asherman's syndrome* - Characterized by **intrauterine adhesions** or scarring, often following uterine surgeries like D&C. - These adhesions can prevent the proper shedding of the endometrium, leading to **secondary amenorrhea** after previously established menses. *Sheehan's syndrome* - Occurs due to **ischemic necrosis of the pituitary gland** following severe postpartum hemorrhage, typically presenting with failure of lactation, fatigue, and **secondary amenorrhea**. - The pituitary damage leads to **deficiency of multiple pituitary hormones**, including FSH and LH. *Turner's mosaic* - While classic **Turner syndrome (45,XO)** is a common cause of primary amenorrhea and gonadal dysgenesis, **Turner's mosaic** (e.g., 45,XO/46,XX) can sometimes result in variable ovarian function. - In some mosaic cases, individuals may experience **menarche** and then develop premature ovarian failure, leading to **secondary amenorrhea**.
Question 5: What is the minimum percentage for normal sperm morphology according to WHO criteria in seminal fluid analysis?
- A. 4 % (Correct Answer)
- B. 8 %
- C. 6 %
- D. 10 %
Explanation: ***4 %*** - According to the **World Health Organization (WHO) 2010 criteria** (maintained in WHO 2021, 6th edition), a minimum of **4% normal forms** is considered the lower reference limit for **sperm morphology**. - This seemingly low percentage reflects the **strict criteria (Tygerberg's strict criteria)** used for assessing sperm shape and structure, which evaluates the head, midpiece, and tail dimensions. - Values ≥4% are considered within normal range for **male fertility potential**. *8 %* - An 8% normal morphology would be considered **above the lower reference limit** according to current WHO guidelines. - While quantitatively better and indicating good sperm quality, it is not the *minimum* threshold required for classification as normal. *6 %* - A **6% normal morphology** is above the 4% minimum threshold set by WHO for normal sperm morphology. - This value is not the designated **lower reference limit** for identifying normal morphology as per the standard recommendations. *10 %* - A 10% normal morphology indicates **very good sperm morphology**, well above the lower reference limit. - However, the question asks for the **minimum percentage** for normal classification, and 10% is not that lower threshold.
Question 6: Which of the following instruments are used in the caesarean section? 1. Bard-Parker blade 2. Doyen's retractor 3. Cusco's speculum 4. Allis forceps 5. Shirodkar's uterine clamp 6. Green Armytage forceps
- A. 1,2,3,6
- B. 1,2,5,6
- C. 1,2,4,6 (Correct Answer)
- D. 1,2,3,5
Explanation: ***Correct: 1,2,4,6*** - **Bard-Parker blade** (scalpel) is used for making the abdominal and uterine incisions in caesarean section. - **Doyen's retractor** is a common abdominal wall retractor used in C-sections to provide good exposure of the uterus. - **Allis forceps** are used to grasp and hold tissues, often the rectus sheath or uterine edges, for traction or approximation during the procedure. - **Green Armytage forceps** are specialized obstetric forceps primarily used to clamp the uterine edges after incision to control bleeding. *Incorrect: 1,2,3,6* - This option incorrectly includes **Cusco's speculum**, which is a vaginal speculum used for gynecological examinations and procedures like colposcopy or Pap smears, not for a caesarean section. - While Bard-Parker blade, Doyen's retractor, and Green Armytage forceps are correct, the inclusion of Cusco's speculum makes this option incorrect. *Incorrect: 1,2,5,6* - This option incorrectly includes **Shirodkar's uterine clamp**. Shirodkar's procedure refers to a type of cervical cerclage, and there isn't a widely recognized "Shirodkar's uterine clamp" used in standard caesarean sections. - Bard-Parker blade, Doyen's retractor, and Green Armytage forceps are correct, but the presence of Shirodkar's uterine clamp makes the option incorrect in the context of a typical C-section. *Incorrect: 1,2,3,5* - This option incorrectly includes both **Cusco's speculum** and **Shirodkar's uterine clamp**. - As explained, Cusco's speculum is for vaginal examination, and Shirodkar's clamp is not a standard instrument for caesarean sections.
Question 7: What is the normal cervical length?
- A. 10 cm
- B. 5 cm
- C. 7 cm
- D. 3 cm (Correct Answer)
Explanation: ***3 cm*** - The **normal cervical length** in a non-pregnant woman typically measures **3-4 cm**, with **3 cm** being the commonly cited average. - During pregnancy, cervical length is monitored via transvaginal ultrasound, and a length ≥3 cm is considered reassuring for pregnancy maintenance. - This measurement is crucial for assessing the risk of preterm labor and cervical incompetence. *10 cm* - A cervical length of **10 cm is anatomically impossible** and not consistent with normal female reproductive anatomy. - The entire uterus (fundus to external os) measures approximately 7-8 cm in a non-pregnant state, making 10 cm for cervix alone unrealistic. *5 cm* - While **5 cm is within the upper range** of normal cervical length, it is longer than the typical average. - Cervical length can vary between 3-5 cm in healthy women, but **3-4 cm is most commonly cited** as the standard reference. *7 cm* - A cervical length of **7 cm is longer than normal** and would be considered abnormally elongated. - This measurement approximates the entire uterine length (fundus to external os), not just the cervix.
Question 8: Which of the following symptoms are seen in endometriosis? 1. Infertility 2. Dysmenorrhea 3. Vaginal discharge 4. Vaginal bleeding
- A. 2,3
- B. 1,2,4
- C. 3,4
- D. 1,2 (Correct Answer)
Explanation: ***Correct: 1,2 (Infertility and Dysmenorrhea)*** - **Infertility** is present in 30-50% of women with endometriosis, making it one of the most common presentations. Caused by inflammation, adhesions, altered pelvic anatomy, and inflammatory mediators that impair reproductive function. - **Dysmenorrhea (painful menstruation)** is the hallmark symptom of endometriosis. The pain is typically severe, progressive, and occurs due to cyclic bleeding from ectopic endometrial tissue, causing inflammation and irritation of surrounding structures. - These are the two most characteristic and consistent symptoms of endometriosis. *Incorrect: 2,3* - While dysmenorrhea is correct, **vaginal discharge is NOT a characteristic symptom of endometriosis**. Vaginal discharge is typically associated with infections (vaginitis, cervicitis) or other gynecological conditions, not endometriosis. *Incorrect: 1,2,4* - While infertility and dysmenorrhea are correct, including "vaginal bleeding" makes this option less accurate. Although some women with endometriosis may experience menorrhagia or irregular bleeding (particularly with adenomyosis or ovarian endometriomas), **abnormal vaginal bleeding is not a primary or pathognomonic symptom** of endometriosis. *Incorrect: 3,4* - **Vaginal discharge** is not associated with endometriosis. - **Vaginal bleeding** as a standalone symptom is not a primary feature of endometriosis, though menstrual abnormalities can occasionally occur. **Note:** Other classic symptoms of endometriosis include dyspareunia (painful intercourse), dyschezia (painful defecation), and chronic pelvic pain.
Question 9: A female patient having frothy vaginal discharge was found to have a strawberry cervix. Which of the following is the drug of choice?
- A. Cefixime
- B. Tetracycline
- C. Metronidazole (Correct Answer)
- D. Fluconazole
Explanation: ***Correct Option: Metronidazole*** - The combination of **frothy vaginal discharge** and a **strawberry cervix** (colpitis macularis) is highly indicative of **trichomoniasis**, caused by *Trichomonas vaginalis*. - **Metronidazole** is the drug of choice for treating trichomoniasis, effectively eradicating the protozoan parasite. - Alternative: **Tinidazole** is also highly effective for trichomoniasis treatment. *Incorrect Option: Cefixime* - **Cefixime** is a third-generation cephalosporin antibiotic primarily used to treat bacterial infections, particularly **gonorrhea** (*Neisseria gonorrhoeae*). - It is not effective against parasitic infections like **trichomoniasis**. *Incorrect Option: Tetracycline* - **Tetracycline** is a broad-spectrum antibiotic commonly used for bacterial infections like **chlamydia** and certain atypical organisms. - It is not indicated for the treatment of **trichomoniasis**, which requires antiprotozoal therapy. *Incorrect Option: Fluconazole* - **Fluconazole** is an antifungal medication specifically used to treat **yeast infections** (vulvovaginal candidiasis caused by *Candida* species). - It has no activity against the protozoan parasite *Trichomonas vaginalis*.
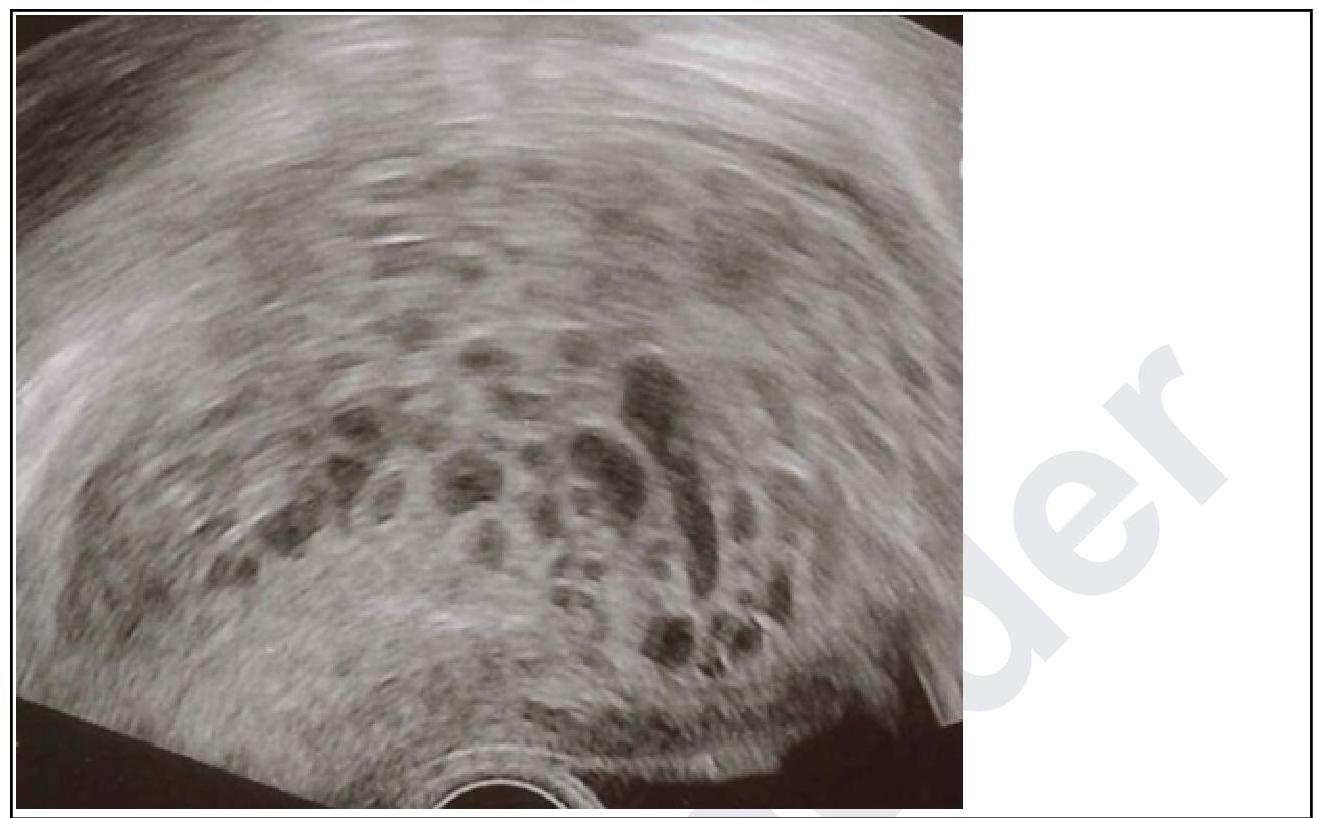
Question 10: A primigravida in her 10th week of gestation presents with spotting. On examination, the uterus corresponds to 12 weeks. Transvaginal ultrasound was done and it is given below. What is your diagnosis?
- A. Blighted ovum
- B. Ectopic pregnancy
- C. Hydatidiform mole (Correct Answer)
- D. Missed abortion
Explanation: ***Hydatidiform mole*** - The ultrasound image shows a **"snowstorm" appearance**, characterized by multiple echogenic vesicles or cystic spaces within the uterine cavity, which is pathognomonic for a hydatidiform mole. - The clinical presentation of **vaginal spotting**, a uterus size **larger than expected for gestational age** (12 weeks uterus size at 10 weeks gestation), and possibly elevated hCG levels (though not given here) are all highly suggestive of a molar pregnancy. *Blighted ovum* - A blighted ovum, also known as an anembryonic pregnancy, involves a **gestational sac without an embryo**. - The ultrasound typically shows an empty gestational sac and does not feature the characteristic "snowstorm" pattern of a hydatidiform mole. *Ectopic pregnancy* - An ectopic pregnancy occurs when the **fertilized egg implants outside the uterus**, most commonly in the fallopian tube. - The ultrasound would typically show an **empty uterus** and a gestation outside the uterine cavity, usually with a mass in the adnexa, which is not seen here. *Missed abortion* - A missed abortion is characterized by the **death of the embryo or fetus but retention** within the uterus. - Ultrasound would show a **fetus without cardiac activity** or a gestational sac that is smaller than expected, without the typical vesicular pattern of a mole.